

Setting the Theme
Following the French Revolution health was added to the rights of people and was assumed that health citizenship should be a characteristic of the modern democratic state. Methods for assessing the strength of the state by counting the population became a new state characteristic. Arguably, the human body has been brought twice over into the market: first by people selling their capacity to work, and second, through the intermediary of health. Consequently, the human body enters an economic market as soon as it is susceptible to diseases and health.[1]
In Indian context, with the advent of European medicine, the harnessing of the new medical knowledge to general well being and public service became evident since the foundation of first medical school in British India, Native Medical Institution (NMI, 1822). What was a medical benevolence of the highly visible earlier sovereign feudal power in India became the new disciplinary power of colonial modernity. It signified a perceptive change in the interplays of state power and their attendant effects on institutions, including medical ones.[2] All these happenings led to the reconstitution of old feudal Indian states to the new emerging nation state.
After the introduction of the Permanent Settlement Act (1793) “many of the older zamindars sold their lands to the new urban commercial elites who had successfully made the transition from Mogul to English rule.”[3] As a result, “the control in the rural area was passing from a Persianized worldview to one that more receptive to English conquerors.”[4] This paradigmatic shift in worldview was quite conducive to the reception of Western medical knowledge, as we shall see shortly. But, to note, the impact of this worldview was limited mostly to the upper echelon of society. Indigenous practitioners were not much affected by this change for a long time (at least till the last quarter of the nineteenth century). This proposition is further strengthened from a report by Meer Ali in 1868 in the Indian Medical Gazette – the mouthpiece of Western medical practice of the time in India. He was a lecturer on practice of medicine at the Medical School of Agra. He reported – “In my professional career I have often observed the successful treatment of dysentery by the hakims of Upper India. They often cure the disease simply and effectually by means of aperients, mucilaginous drinks, and light farinaceous food.”[5]
At a later period, it became once again evident from a report which made a plea to indigenous practitioners. It was intended that all other competing knowledge systems would be assimilated into and subsumed within one overarching system of Western medical knowledge. If, the report argued, everything goes in uniformity with the prescriptions of this report – “in place of the present double system of medicine practiced in India, we will have Western science engrafted on Eastern customs and requirements, the fusion of the two being far more in accordance with the value and wishes of the people than other systems separately.”[6]
In the parliamentary battle of 1813 the free-traders had stripped the East India Company of its commercial monopoly over India. “Free trade was its solid foundation. Evangelicalism had provided its programme of social reform, its force of character, and its missionary zeal.”[7] Moreover, “Utilitarian hopes of inaugurating a competitive society based on individual rights in the soil, depended as much upon the revenue assessment, and the registration of landholdings which accompanied it, as upon the superstructure of judicial codes and establishments.”[8] Regarding the year 1818, Stokes reminds us – “As Shelley wrote in that year in his preface to Prometheus Unbound, the cloud of mind was discharging its collected lightning … that the orator of the new liberalism, the young Macaulay, shook off his father’s toryism and avowed himself a Radical. It was in the same year that James Mill published his great History of British India, and became a candidate for high office in the Company’s Home Government.”[9]
All these phenomena, taken together, led to a situation where Macaulay was backed by the great bulk of Calcutta mercantile community in its fight for English education. It was the period gestating the formation of semi-modern Indian state. In tandem, changes occurred in education policy – a constituent part of which was medical education. Medical education historically became one of the most productive imperialist networks through which benefits of imperialism could be visible. In England, there were circumstances in which social resentment and political radicalism could flourish; during the 1839s and 1840s a British revolution seemed a real possibility. The social upheavals and ideological currents flowing from the revolution impinged medicine in a variety of ways.[10] The foundation of the University College London (UCL) in 1826 influenced to a great extent the formation and architecture of the CMC. UCL was to become a site at which “crucial issues of orthodox medical knowledge and of the locus of medical authority were contested.”[11] This institution was secular, ‘infidel’ to its detractors, and put emphasis on the importance of basic sciences, and practical experiments. “It did not impose some form of religious test (as in Oxford and Cambridge universities) on those who wished to study there.”[12]
Metaphorically speaking, the first cadaveric dissection (28 October, 1836) had become successful to transform colonial medical anxiety to secular self-confidence. David Hare was quite apprehensive to see the project of the first dissection finally brought about and settled without opposition. A few days before the first dissection, he anxiously asked Madhusudan Gupta – “Do you not know what amount of pain and anxious thoughts you have kept me in for a week almost? … Have you found the text in your shaster authorizing the dissection of dead bodies?”[13] Gupta’s reply was affirmative. He did not fear any opposition. He told Hare, “I and my Pundit friends are prepared to meet them if they come forward which I am sure they will not do.”[14] But, in actual reality, the first demonstration by dissection caused great anxiety in society.[15] The College gates were closed to prevent forcible interruption of that awful act.[16]
Lord William Bentinck had his brief stint in Calcutta from 1828 to 1835. During his rule, he played a key role in the transformation of Indian administrative, educational, tax patterns and, to an extent, social ambience of Calcutta. Bentinck was a Whig in politics. The “avowed” radical Macaulay and liberal James Mill joined him. Macaulay was highly articulate representative of the “West European liberal intelligentsia whom we generally associate with the British Reform of the 1830’s and the revolutions of 1848.”[17] Though the Calcutta mercantile community had its own narrower, more selfish standpoint, Stokes argues, “Substantially it swelled the great tide of liberalism engulfing the English mind in the eighteen-thirties.”[18] Importantly, despite the spread of Utilitarian philosophy and Evangelism to an extent, the indigenous cultures of India lingered on in the courts of the princes and pensioners.[19] Bentinck’s later “encouragement of capitalist enterprise in India owed at least as much to … political economy or Benthamism.”[20] In recent scholarship, it is argued that the symbiotic relationship between India’s nascent capitalist and gentry classes and the East India Company started to come under new pressures during the first quarter of the nineteenth century.[21] The shift in relations between the British and Indian capital and the transition to a “new capitalist order in India was most closely associated with governorship of Lord William Bentinck.”[22]
These changes and developments in Indian society during the 1830s, when contrasted with Charles Maclean’s monopolist mercantile views in 1813, make one understand the economic and social transition in a better way. Charles Maclean asked the “real and only question” – “What would be the consequences of laying open the navigation to India to private ships?”[23] In his opinion, it might even lead to the commercial bankruptcy. Contrarily, Bentinck is known to have said, “The sooner however that some old-fashioned principles are thrown overboard the better…”[24] Between 1829 and 1835, he transformed a budget deficit of one and a half million pounds sterling into a surplus of half a million pounds. Bayly emphasizes, “It is against this background that Bentinck’s educational reforms must be set.”[25] Moreover, from 1819 new influences were at work at India House “with the appointment of James Mill, the Utilitarian philosopher, as assistant to the Examiner of India correspondence.”[26]
Bentinck reached Calcutta at a time when all these happenings (the strife between the monopolist EIC and the rising Bengali mercantile community advocating for free trade and other issues) “were a matter of lively debate both there and, because of the coming need to renew the company’s Charter at home.”[27] To add, Bentinck had also a copy of Panopticon of Bentham in his possession. Bentham wrote, “While writing, it occurred to me to add a copy of a work Panopticon; the rather because, at the desire of Mr. Mill, it is in the hands of your new Governor-general, Lord William Bentinck…”[28] The famous Panopticon is a historical signifier of the emergence of normalizing disciplinary power (as contrasted with blatant coercive power of pre-modern parochial state) on the one hand, and a sovereign state on the other. Moreover, Bentinck had “indeed subscribed in 1826 for two shares in the newly founded University College, London – an institution under combined Whig, Benthamite and Dissenting control, and a forward battalion in the ‘march of mind’…”.[29]
Another notable change during the period was the introduction of clock-time in everyday life as well as in administrative services. “Disciplinary time was a particularly abrupt and imposed innovation in colonial India. Europe had gone through a much slower and phased transition spanning over some five hundred years: from the first thirteenth- fourteenth-century mechanical … Colonial rule telescoped the entire process for India within one or two generations.”[30] The making of a new kind of individual and, accordingly, the reshaping of everyday Indian life was in the offing. CMC turned out to be a tool to have facilitated the making of this modern state in so many ways. Bayly informs us, “Physicians were, in addition, important information gatherers for the state.”[31] Those who resided in cities held regular councils and could frame broad calculations of mortality rates by ordering the custodians at the city gates.
In a private letter to his friend Peter Auber on 12 March 1834, Bentinck commented, “Three thousand boys are learning English at this moment in Calcutta and the same desire for knowledge is universally spreading … My firm opinion on the country is that no dominion in the world is more secure against internal insurrection …”[32] Interestingly, the passion for acquiring English education provided the state its much desired internal security. Thus modern medical profession and education, which was then a part of general education, played a significant role in the making of the burgeoning ‘modern’ state.
Brief Review of Pre-CMC Medicine and Society
In February 1835, a memorial signed by 6,945 Hindu habitants of Calcutta, including all the managers of Hindu college, the parents and guardians of the students of English, was presented to Bentinck praying that the existing restrictions on the use of the English in the law courts be abolished.[33] It signifies that somewhat “universal” acceptance of English as the primary administrative language of the newly emerging modern state was phenomenally palpable. The most important educational feat of Bentinck was the foundation of the CMC. To be sure, CMC had ushered in “hospital medicine” in India. Hospital medicine itself was a new phase of development in the evolution of medicine, as distinct from its earlier phase ‘bedside medicine”. Disease appeared to being located within a three-dimensional body – symptom > illness > sign. Depth or volume of the body – the 3rd dimension – was added to symptom > illness perception whereby the body emerged to be of three-dimensional nature. Doctors were, then, to extract sign, i.e. pathology inside the body. Pictures shown below would help us to get at the point.
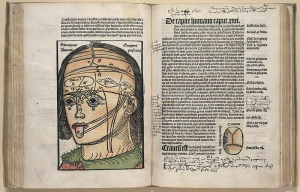
Fig. 1 Magnus Hundt’s Antropologium de hominis dignitate, natura et proprietatibus, de elementis, partibus et membris humani corporis. (Leipzig: Wolfgang Stöckel, 1501). [Antropologium, published in Leipzig in 1501, serves to explain the body not only anatomically and physiologically, but philosophically and religiously too. Humans were created in the image of God and represent a microcosm of the world as God created it.
Courtesy: Historical Anatomies on the Web, National Library of Medicine, US.]
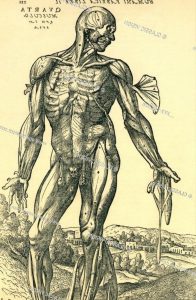
Fig. 2 Three-dimensional body and its different muscles layers accurately shown.
[From Andreas Vesalius’ De corporis humani fabrica libri septem. (Basel: Johannes Oporinus, 1543): 368. He was the anatomist to illustrate human body and its internal organs in a truly three-dimensional way and without any religious or philosophical connotations.]
The perception of this particular 3rd dimension or the depth/volume of the body was altogether absent in traditional healing systems like Ayurveda, Unani or Siddha. As Ackerknecht has aptly put it – “it was only at the hospital that the three pillars of the new medicine – physical examination, autopsy, and statistics – could be developed.”[34] One of the key features of hospital medicine – pathological anatomy – was cultivated in Paris too.[35] In his acute observation, Ackerknecht notes, “These were essentially a consequence of the tremendous influx of uprooted and penniless boys and girls from the country and of the beginnings of the Industrial Revolution.”[36]
How was the medical and health situation in India, especially in Bengal, during the period we are talking about? It was reported, “We have ourselves witnessed many harrowing cases of natives killed outright, solely through the barbarous treatment of the Kabiraj, or village-doctor, who knows far less about curing diseases than an English farrier does; and yet this Eastern type of Dr. Sangrado (a character after Doctor Sangrado, physician, whose panacea was copious bloodletting and drinking of hot water, in the picaresque novel Gil Blas – L’Histoire de Gil Blas de Santillane, published between 1715 and 1735 – by Alain René Lesage, French novelist and playwright who died on 1747) requires a fee of one rupee in many cases from poor fellows, who earn only four rupees a month!”[37] This was a space outside the realm of modern state and modern medicine as well in their traditional ‘dispositif” of living. Hence, to mitigate health and medical problems and, purportedly, to insinuate the tentacles of modern normalizing power, it was suggested at a later period, “a class of pupils to be instructed through the Bengali language (in the CMC), many of whom might be attached to the different thannas.”[38] Thus, medicine which reached even the most interior and remote parts of indigenous social lives attained benevolent face of the modern colonial state. Interestingly, in this process of making Western medicine humane and devoted to the alleviation of sufferings of poor Indian people, the ‘social’ (of indigenous life world) thus became tenuously tied to the ‘state’ (unlike the ‘individual’ of modern European state) with the aid of modern Western medicine. Ironically, the ‘social’ was transformed into a new kind of individual when housed in the hospital ward as a ‘case’.
It was the Act of 1833 in England that injected “fresh vigour into both the Home and Foreign divisions of [the] oriental administration… [and] medical and general education began to experience something like the attention it deserved”.[39] S. Goodeve Chuckerbutty, one of the brightest students of the CMC and the first Indian to excel in the IMS examination, wrote in 1864, “The Kabirajes were ready enough with their nostrums whenever they were required … Of human anatomy they were utterly ignorant; consequently, their surgery was of the rudest kind.”[40] Examples may abound. But the basic fact remains that the state of medicine as a whole was not much laudable before the advent of Western medicine with its institutional practices.
We can have a good account of deplorable medical condition of rural India during the time CMC was founded. Montgomery Martin did extensive surveys of rural Bengal, Bihar and Assam. In the surrounding areas of Rajmahal, he found about “20 Jurrahs, who evacuate the water of hydrocele, treat sores, and draw blood both by cutting a vein, and by a kind of imperfect cupping. They are by birth barbers.”[41] On the contrary, medicine was practiced by Brahmins or Vaidyas or Kayasthas. “Medicine (Baidya-sastra) is taught by several of the pundits, some of whom also, although they grammarians, practice the art.”[42] In Darbhanga, he found some untrained medical men doing their business with herbs. They were variously called as “Atai Baidyas, or doctors defraud the ignorant; Dehati Baidyas, or village doctors; Chasa Baidyas, or plough doctors; Haturya Baidyas, or doctors who attend markets.”[43]
In another area he found 53 Hindus and 4 Mohammedans “profess the art (of medicine)”.[44] Montgomery Martin is possibly the first Company surgeon to talk about, in 1838, what we now know as lathyrism. He observed, “It seems to consist in a weakness and irregular motion of the muscles moving the knees, which are bent and moved with a tremulous irregular motion, somewhat as in the chorea, but not so violent. … It is attributed by some to eating khesari (lathyrus-sativus); but this seems fanciful …”[45] In adjacent areas of Purnea, he found about “150 Jurrahs, or surgeon-barbers, who cup, bleed, and treat sores. The midwives are of the lowest tribes, and merely cut the umbilical cord.”[46] He found that there remained some acts of ‘hybridization’ of European inoculation and Indian variolation. “I have heard that some Europeans have been silly enough to employ them to repeat their spells, even when an European surgeon had performed the operation.”[47] We should note that while the scholastic practice of medicine was vested in the hands of the high caste people, surgical procedures were relegated to the lowest caste and Muslims. The division between medical and surgical practices is quite evident from the big demographic survey done by Martin.
Importantly, Ainslie found Hakeems who possessed a great deal of information, and were, “in general, men of polite manners, unassuming, liberal minded and humane.”[48] If those people, living beyond the reach of the modern state, could be brought under the surveillance of local dispensaries and made to learn the techniques modern hygiene, sanitation and other health programs of the modern state would secure its meaningfulness. Such programs were actively taken by the colonial state. Medicine turned out to be an effective tool in the making of state. As can be easily understood, with the increase of the armies in the three Presidencies and the increase of factories and stations the medical department increased in numbers.
In 1824, some people of Calcutta wrote to the editor of the Sangbad Coumudy (the Moon of Intelligence), “The people of this country have been relieved from a variety of diseases since it has been in the possession of the English nation.”[49] They wrote that the ten rupees which poor people earned every month was barely sufficient to sustain the family, and, consequently, “the populace have generally not the means of calling in a European doctor … whereby the poor might avail themselves of the medical treatment of European doctors”.[50] They argued, “Were the Hindoo physicians to instruct their children in the knowledge of their own medical Shasters first, and then place them as practitioners under the superintendence of European physicians, it would prove infinitely advantageous to the Natives of the country.”[51]
According to the reporting, this endeavor would benefit the society in four ways. First, pupils would be acquainted with both the English and Bengali mode of learning. Second, “by going to all places, and attending to poor as well as rich families, and to persons of every age and sex, he could render service to all”. Third, “he could go to such places as were inaccessible to European doctors”. Fourth, “this kind of medical knowledge, and the mode of treatment by passing from hand to hand, would be at length spread over the whole country”.[52] The new medicine, heralding its universality with the words “[for] every age and sex”, also incorporated a kind of secular nature into it. To emphasize at this juncture, ontologically speaking, the existing predominant medical practice of the time, Ayurveda, does have unwaveringly male gaze.[53] Bearing only the faint trace of the gurukul system in which knowledge could be passed “from hand to hand”, the English mode of teaching had to be incorporated for better efficacy.
Further, “The demand thus created gradually drew large number of practitioners of European medicine into the villages in the mofussil, and every outbreak of cholera or fever to a noticeable extent in any locality increased their numbers.”[54] From a Foucauldian viewpoint, it may be deduced that the clinical gaze extended from metropolis to the periphery. Indian society experienced the emergence of a new type of medicine which was not only patronized by the state (as was not in case of Ayurveda or Unani) but also actively set it into operation.
Experiments like stipendiary education and, to emphasize, the intertwining of medicine and surgery in one person – one of the hallmarks of “Hospital Medicine” – were effectively practised at the CMC. Moreover, CMC was (1) the first modern institution in India to introduce residential education and (2) to send students to England/Europe for higher education.
Another significant event in 1840s was the departure of four of the College’s students[55] for additional study in London. As soon as the success of the students in anatomy and chemistry was demonstrated, the faculty laid their reputations on the line again by calling for chance to see what their students could accomplish in competition with English students on English soil. Bramley was the first[56] to request permission for this, and O’Shaughnessy the second to do so.[57] But the Court of Directors quashed these aspirations, and it remained for Goodeve to be successful. With grudging government financial support, but more from the private Indian and English sectors of Calcutta, the four students in company with Goodeve set sail for England on 18 March 1845, appropriately enough aboard the Bentinck. They enrolled in University College London.
Gorman notes three important effects of this sojourn. First, it showed in a dramatic and conclusive manner that Indians could master science and medicine on a level with Europeans. Second, after these students received their degrees from the University of London and their diplomas from the Royal College of Surgeons and returned to India, they served as disseminators of modern science and became role models for future Indian scientists. Lastly, their example set the stage for a veritable flood of Indian students to England for study in all fields, a movement which continues to this day, Gorman comments, “The British had invaded and conquered India politically and geographically, but now the Indians had done so in England academically.”[58]
Another point of importance may be cited here. Arnold comments, “The fruits of O’Shaughnessy’s enquiries, backed by laboratory experiments, post-mortem analyses, conversations with vaids and familiarity with local medical practice as well as metropolitan medical jurisprudence, were incorporated into his Bengal Dispensatory and Bengal Pharmacopoeia.” But government was not receptive to these internationally acclaimed works. They were more interested “in the application of chemistry to the neds of trade and industry (such as assessing the suitability of Indian clays for making firebricks and other ceramic goods currently imported at great cost).”[59] As a result of these meta-scientific works O’Shaugnessy was given the additional title and extra remuneration of the Chemical Examiner in June 1840.[60] The interest and inquisitiveness of a scientific mind and the interests of the state fell apart, as almost always happens historically.
Consequently, CMC itself was itself a truncated replica of University College London or other premier medical institutions of Europe. Unfortunately, in 1840s and, also later on for quite some time, CMC was confined within the cocoon of ‘hospital medicine’ – post-mortem dissection and clinical teaching, but not any laboratory-centered physiological researches – failing to transcend into the higher level of scientific studies and experimentation. Most likely, the primary cause was that colonial authorities wanted only capable practitioners for their daily chores of medical requirement, but not capable practitioners as well as capable enquirers at all. It happened that medical education at CMC was shaped by a variety of educational and political circumstances in each country – in India it was undoubtedly was colonial interest. Unlike O’Shaughnessy’s classes, the students were not encouraged to ask why. On the other hand, they were made to be good, docile, disciplined and obedient citizenry for the colonial state.
From another perspective, Bentham’s Panopticon via Bentinck and Auckland reached out to heterogeneous Indian society. Medicine, like state, became the homogenizing process. One example of how medicine and state were tied up happily with this bred newly citizenry during the days of the Great Mutiny (1857) was provided by Chuckerbutty – “Out of the large body of Native Doctors and Sub-Assistant Surgeons who have issued from this institution (CMC), only two or three have been proved to have actually joined the ranks of rebellion, although the vast majority of them were exposed to the same temptations as the sepoys of their regiments.”[61]
To emphasize, the twin need for an educational economy as well as a cohort of trained “native doctors to supply vacancies in regiments”[62] was the principal motive behind educating ‘native doctors’ in India. In 1855, the Lancet reported, “It is little more than thirty years ago since the wants of the army caused the Medical Boards of Madras and Calcutta to commence instructing natives in some of the simple varieties of medical knowledge”, though these were “of the humblest possible description.”[63] The economic need of the state was explicitly stated: “Native surgeons, educated at the Company’s Medical College in Calcutta, could be easily procured, and would be glad to be employed, at from Rs 25 to Rs 50 per month, with rations and a free passage.”[64] For each English soldier, on the other hand, it would cost the state £100 to train him for duty.[65]
To emphasize, modernity in India was operating in an asymmetrically overdetermined space. The flow of knowledge was always from the centre like London to its recipient periphery Calcutta or Bombay or Madras. For a limited period in the early years of colonialism there were some exchanges of knowledge, but as the colonial state consolidated its power it became a one-way journey.[66] It should be mentioned that the way Indian vegetables, minerals and animal products were regarded by earlier authors like Ainslie as “Materia Medica of the Native Indians”[67] was completely reversed after the formation of the CMC. In his “Introductory Address” at the CMC on March 17, 1836, Principal Bramley commented, “there can be no question that your materia medica contains many articles of a fantastic, useless, or destructive character, of which further advance in European Science will point out to you the mischief and danger.”[68] At the same session, Goodeve noted, “Hitherto you are ignorant of the science of materia medica; you know not the names, much less the properties of the various drugs which you are employ in the cure of disease…”[69]
It became widely accepted that “the British government could not have established an institution calculated to be of greater benefit…than the Native Medical Institution [NMI]”.[70] Macaulay’s efforts seemed only to add a snowballing effect to the process already started by the students of the NMI and Calcutta elites taken together. During the decade of its existence, the number of native doctors “which this institution furnished to the public service between 1825 to 1835 … was 188”.[71] Eight of the pupils “who had been educated in this seminary were appointed native doctors, and sent with the troops serving in Arracan”.[72]
My contention is that the brief phase of the NMI and the medical classes at the Calcutta Sanskrit College represents the period of gestation of hospital medicine in India. Medical classes at the Sanskrit College started in 1827. But the preparatory phase to introduce pupils to modern science – its technology and technique – had begun earlier. The report of 1828 stated that the progress of the students of the medical classes had been satisfactory “in the study of medicine and anatomy; and particularly that the students had learned to handle human bones without apparent repugnance, and had assisted in the dissection of other animals”.[73] They also “performed the dissection of the softer parts of animals’, and opened ‘little abscesses and dressing sores and cuts”.[74] Moreover, at the Sanskrit College the number of pupils was then 176 and the number was quite impressively increasing. Of these 176, only ninety-nine students received allowances from the college.[75] This estimate makes it clear that seventy-seven students were without allowances and still pursuing their studies at their own expense – the lure of English medical education can be unmistakably discerned from these facts.
In the first quarter of 1832 a hospital was attached to the Sanskrit College “required for the use of a Native Hospital and Dispensary.”[76]
Gradual exposure to dead bodies began to erase the social taboo against touching the dead. Before the foundation of the CMC, students were exposed to the postmortem examination through attending clinical classes at the General Hospital. Once again to remember, this act prepared the environs for exposing the new generations of pupils to visual, auditory, verbal and psychological acculturations with the new culture of medicine consistent with the functioning of the new state in the making. Along with these, moral, behavioral and clock-time acculturations were also introduced. These acculturations were of paramount importance as it paved the way for the emerging new medical individual and new citizen as well who would be disseminating new knowledge of the state as well as become its flag bearers.
Hospital Medicine in the Making of Modernity and Modern Citizenry
One of the profound changes brought about by the G.O. No. 28 of 28th January, 1835 (foundation of CMC) was the introduction of secular nature of medical education, not “inferior to some of the most celebrated schools of medicine in Europe”. In 1815, it was reported, “a Brahman boy would not sit down on the same mat with one of another caste.”[77] Within 30 years, people of both high and low caste together performed dissection. In 1844-45 session of CMC, there are – “Brahmins, 19; Kaists, 21; Boyddows, 8; Kyburt, 2; Tanty, 2; Bankers, 3; Soory, 1; Talee, 1, Shutgope, 1.” Total number of students was 57.[78] The lectures at CMC started with osteology, leading finally to dissection proper on 28 Oct. 1836. Later on, Medical Jurisprudence and Pathology were added. For better clinical training, two small hospitals – one Male, another Female – were added to the College in 1838. The new kind of midwifery, unlike indigenous one, started since 1840.
Unlike Europe and UCL (fees ranging from £5 to £20), students were stipendiary at the CMC. When stipend was given in CMC, “fee for the Examination” of University of London was £5 (equivalent to Rs.50 at that time), and that of St. Guy’s £20.[79] A mercantile corporation like the EIC invested this amount of stipendiary money not for any gambling out of nothing. It was political economy of education – investment for the generation of desire for European medicine and, consequently, European political hegemony, which led to furtherance of more convincing approval of the British regime as well as the gradual adoption of European medicine and hegemony socially as a token of benevolence.[80]
At the end of 3 and ½ years’ education at CMC – when each candidate had attended 3 courses of anatomy and physiology, 2 of actual dissection, 3 of chemistry, 1 of natural philosophy, 2 of materia medica, 2 of general and medical botany, 2 of practice of physic, 2 of the principles and practice of surgery and 1 of operative surgery – rigorous examinations were taken, spanning from 30 October 1838 to 9 November 1838. Finally, 4 outstanding students (out of 11) were declared successful – Umacharan Set, Rajkisto Dey, Dwarakanath Gupta and Nobinchunder Mitter. They were appointed as sub-assistant surgeons in new dispensaries.[81] It should be emphasized that within 8 years of the first dissection which was performed with utmost secrecy the situation changed completely. It was firmly stated – “Every dissecting student shall deposit a sum of two Rupees in the Office of the College, to make good any loss or unnecessary destruction of instruments.”[82]
Along with this, on March 16 1841, it was gleefully noted – “We are happy in being able to report an increasing desire, on the part of the native community, to obtain Medical aid, and in proportion as the purposes of the Dispensaries become known, their advantages will be more and more appreciated.”[83] In 1847, Balfour felt that one of the most striking features was the wonderful success with the opening of Dispensaries. Dispensaries were held by the great majority of the people with increasing favour. They were manned by graduate sub-assistant surgeons of the CMC. Sykes reported “267,456 cases treated”, who were relieved in the Charitable Dispensaries of India in 1847.[84] Arguably, the era of modern public health began to emerge.
Practitioners required by Government made available for the different services required and eventually when subordinate seminaries were to be established in different localities it would become an aim that the most promising students might become a professor – “the College may become a normal Seminary through which individuals capable of conducting schools of Medical Education in different parts of the Country may be provided.”[85]
Notably, ether anaesthesia was administered on 22 March 1847, while chloroform was applied on 12 January 1848—within two months after its first introduction in London.[86] Among the prominent points of interest referred to “were the extraordinary success of some of the graduates of the College in the performance of the formidable operation of lithotomy, and the valuable results which had followed the introduction of chloroform into the practice of surgery.”[87] Chloroform was given in two obstetric cases of operative procedure with perfect safety and success in the presence of several of professors, and a number of the students of the CMC.[88]
In the early days of the CMC original researches were done in basic sciences – “an amazing total of 557 books and articles with an average of 31 per professor.”[89] However, in the last months of 1868, on the eve of the opening of the Suez Canal, the freedom of British medical doctors in India to keep purely medical considerations uppermost in mind came to an abrupt end and its lingering impact continued until the end of the 19th century. Colonial authorities were not in a position to encourage/allow free scientific inquiries in colonies like India.[90]
Harrison, in one of his monographs, concludes thus, “The emergence of what contemporaries celebrated as “rational or “scientific” medicine was therefore intimately bound up with Britain’s commercial and imperial interests, with the empire at home as well as overseas.”[91]
Sometimes there appeared true scientific spirit and rational enquiry suited to colonial soil. W. B. O’Shaughnessy was one of the very few progenitors of such acutely sensitive free scientific mind. But true scientific spirit (except some hands-on training) was subsumed by the Utilitarian leitmotif of the day. And that is undeniably expected when modernity is grafted, not evolving through socio-economic-political changes.
The Making of Navya Āyurveda
In Bengal, it effectively started with the writings of influential Āyurvedic scholar as well as modern medicine-trained Kavirāj Mahāmahopadhyāya Gananath Sen. What may be the most intriguing part of this discussion is the fundamental ontological and epistemological transformations carefully wrought into the matrix of Āyurveda, following its encounter or vigorous exchanges with Western medicine. While in the field of materia medica or mineral or botanical knowledge there was some acceptance of Indian medical knowledge till the early 19th century, after the institutionalization of hospital medicine through the CMC it was completely asymmetrically overdetermined. Āyurveda was now at the receiving end only.

(Kaviraj Mahamahopadhyaya Gananath Sen)
Following Meulenbeld, “The renaissance of āyurveda since about the middle of the nineteenth century – historically a fascinating phenomenon – made its protagonists and epigones feel called upon to sketch a profile of this science that would be serviceable in the competitive struggle with Western medicine.”[92] The question arises how this renaissance was brought into becoming and set into motion. French anthropologist Francis Zimmermann explains, “Only in contemporary times and no doubt influenced by European medicine have the Ayurvedics been concerned with indicating physiological phenomena cartographically. … Through a kind of retrospective rationalization, the image of channels in rice paddy is replaced by a modern image, one familiar to any twentieth-century high-school student; namely, the anatomical diagram, which illustrates the ancient text without affecting its mode of thought: digestion remains an irrigation.”[93]
It may be benefitting to mention here that at least since 600 A.D., the study of anatomy and surgery had almost ceased to exist in India.[94] The scholastic practice of Āyurveda was solely confined to medicine, while surgical crafts were relegated to the hands of low-caste people. Zimmermann provides an example of virtual application of surgical knowledge by present day Āyurvedic practitioners. To the high-caste physicians who have access to Sanskrit knowledge the chapters on surgery and midwifery are a dead letter. Nevertheless, “the learned practitioners do read and recite these Sanskrit texts by heart so that apparently there will be no break.”[95] Modernization of Āyurveda tried its best to reconcile these two irreconcilable acts thorough novel ideas and perseverance.
Much later after the foundation of the CMC and ramifications of dispensaries to instil invisibly the techniques of governmentality and protection and creation of new selves among themselves, British authorities did suffer from anxieties in the sense that the victorious triumph of modern medicine was not thorough. In 1867-68, in one estimate there was one trained medical men to every 4,285 of the general population.
Talking about indigenous practitioners it was reported, “In native society, all over the country, these men still hold their own, and are greatly respected, ministering as they do to the troubles of both body and mind of the people, and generally possessed of a superior education … Under British rule, however, they have disappeared altogether from political life, and socially have little or no standing in European society, where they are virtually ignored.”[96] Moreover, “Besides the element of superstition, there are other causes that separate the European from the Native practitioner. Both Hindoos and Mahomedans cling with blind obstinacy to the theoretical dogmas of the ancient fathers of medicine; and there is not much wonder they do so, for the works of these authors are alone plentiful in a language which they understand. These books too, besides being cheap and compendious, do not require, in order to be understood, any previous study of the elementary foundations of medicine, such as anatomy, chemistry, physiology, &c.: subjects which the native practitioner has seldom the desire or opportunity of acquiring.”[97]
Girindranath Mukhopadhyaya, an eminent Āyurvedic scholar, seemingly in contrast to Gananath Sen, notes, “The Sanskrit College was opened on the first day of 1824. This year forms a landmark in the history of education in India.”[98] According to Mukhopadhyaya, “dissection of the human body” which was “found to be stumbling-block to the progress of the students in Anatomy” was brought to fruition by the Pundit Madhusudan Gupta.[99]
At those moments of nascent nation-state in India, in September 1923, Major R. N. Chopra, Secretary, Ayurvedic Committee, Bengal, sent a set of 17 questions to Girindranath Mukhopadhyaya[100], B.A.,M.D., Bhishgacharya, with the intention to modernize Āyurveda. Girindrnath’s replies decisively clinched the question of modernization of Āyurveda, not limited only to copying from English medical texts or incorporating modern medical theories. It also emulated structured, organized practice of scientific knowledge and modern curricula to make Āyurveda compatible with the changing mode of the state.
It dealt with organizational structures and definite programs to make Āyurveda and compatible with the changing modern world of the time. His recommendations included – (a) “Establishment of hospitals for the treatment of patients according to Āyurvedic system”, (b) “Foundation of charitable dispensaries in rural areas”, (c) “Foundation of a scientific library for the use of the students”, (d) “Translation of Sanskrit books and manuscripts into English … for then only can we expect healthy criticism from the savants of the world”, (e) “The text books as read by the students of Āyurveda require to be recast and re-edited to suit our modern conditions of life”.[101] Moreover, he proposed for “Popular lectures dealing with improvements in hygiene and cognate sciences illustrated by lantern slides, pictures and drawings to elucidate the subject.”[102] He also pleaded for “therapeutic gardens” and “museums”. In his opinion, “The importance of a museum in teaching a scientific subject has been recognized by eminent authorities”.[103] In the Central College, provisions were to be made “for the study of the various sub-divisions of the Āyurveda, namely medicine, surgery, midwifery, children’s disease, pathology, materia medica, anatomy, physiology, hygiene, medical jurisprudence, and the elementary sciences, viz., biology, physics, chemistry, according to the modern scientific methods.”[104]
Hence, to make these indigenous practitioners modern and endowed with modern knowledge of health and healing bore a great importance for Navya-Ayurveda (as I am not aware of Unani or Siddhaa, I shall refrain from commenting on them). Girindranath clearly charted a program regarding Tols (traditional centers of Āyurvedic learning). In his opinion, for the time being “the tol system may be retained … the dual system of study may be followed for a time.” But, according to him, “it must however be clearly borne in mind that sooner the Tol system of medical education be stopped, the better.”[105]
A new hybridized Āyurveda was figured out and set into social motion. Āyurveda was now in the gleeful spirit of mimicry of Western medicine. Girindranath stresses that no medical institution is complete without hospitals – “A complete knowledge of diseases can be acquired in the wards of hospital.”[106] We can understand the overarching impact of modern medicine on Āyurveda.
In Āyurveda, patients were always seen in domestic setting – in patient’s own environment. In this new structure of “modernized” Āyurveda patient’s subjectivity would metamorphose into an object of the wards. Moreover, such new phenomena would lead to making the patients into a cohort for statistical analyses, which was completely unthinkable in traditional Indian medical concept. Girindranath strengthens his logical position by citing reference to the Chāndsi doctors who were specialists in ailments related to pile, fissure and fistula-in-ano etc. For him, “the Chāndsi doctors, who still carry a lucrative trade in Calcutta, are in the habit of keeping patients in their own house in a room called by them ‘hospital’ at their own cost, and thus acquire skill in performing certain surgical operations, e.g., piles and fistula-in-ano.”[107]
Here Girindranath’s observations pose two distinct questions. First, till the time he mentions Āyurveda was basically a scholastic medicine solely dealing with medical problems and confined to high caste people of the society. Moreover, surgery was a taboo to this scholastic medicine and relegated to the low caste. Second, to weave his logic and frame his issue he alludes to the Chandsi doctors who were basically low caste people and somewhat related to Unani system and were looked down upon by scholastic Āyurvedic practitioners. Consequently, in the matrix of Āyurvedic learning some amount of secular characteristics were infused.
Regarding the functioning and curricula of the Central Āyurvedic College, Girindranath proposed a course of four years. He detailed different subjects to be taught in different years. One must remember the curriculum of the CMC in pre-1845 era. In his proposition, subjects were arranged thus for different years. For the students of “First-year” subjects were chosen thus, and similarly in other higher years as well – physics, chemistry, biology and anatomy, dissection and practical training in scientific subjects. For “Second-year” – anatomy, physiology, materia medica, pathology dissection, practical classes, and hospital duty. For “Third-year” – medicine, surgery, midwifery, hygiene, clinical medicine and surgery, labour cases, hospital duty – medical and surgical, and operative surgery. Fourth-year – same as in the third year, medical jurisprudence and history of medicine. Then he comments, “After a few years, it would be found that a five-year course would cover the subjects better than a course of four years.”[108] At this juncture, it would occur to the reader that it was a virtually a replica of the courses taught at the CMC. Even the transition from four to five years was in mimicry of post-1845 curricular changes in the CMC.
Despite all these modernizing efforts, Girindranath was apprehensive of the success of the Āyurvedic doctors of the new breed. In his apprehension, “He shall have to create a demand for medical and surgical skill, where there was no felt no want of them. The pupils, on the other hand, cannot be very enthusiastic – their prospect in life distant and somewhat indefinite.”[109] Moreover, “In private practice, they shall have to fear ridicule and opposition from the Graduates of the Medical Colleges and Licentiates from Medical Schools who may vaunt for their superior knowledge. There are no text books suited to modern times: such books must written in English and vernacular.”[110]
The eternal flow of healing traditions was undermined by the supposed votaries of this tradition itself. It created a kind of ‘epistemological hypochondria’ which led them to vigorously adopting all the means Western medicine, as epitomized in the CMC. Intriguingly, ‘epistemological hypochondria’ in the wider sense of meaning was actually ascribed to the traditional tol system of learning. Girindranath realized that the modern Āyurveda and the tol system would be incompatible. “Tols shall have great difficulty in their practice”, he explains, “So there ought to be a separate system of teachings for those Kavirajes to give them some idea about modern advancements.”[111] Finally, admitting and confining patients into hospitals and dispensaries would facilitate various therapeutic trials. In his words, “I hold that for the present, it is desirable that English language should be the medium of study in the college. It will bring education of the students up to modern standard of method and efficiency ….”[112] The adoption of modern scientific methods, “where necessary for the said purpose and is not based on blind orthodoxy”[113], were also quite expectedly emphasized by him.
Concluding Remarks
To be sure, I am not on the judgmental seat to give verdict whether this entire process was conducive or not to the revival of Āyurvedic learning. But it can be safely said that the rise of hospital medicine in India was instrumental in the total reconstruction of Āyurveda in its core – both epistemologically and ontologically. In this way the reconstruction of Āyurveda was a definite entity and force in the making of modern Indian state. To put it otherwise, modern Indian state became successful to reorient Āyurvedic learning to suit its purposes.
To remember, since the foundation of the CMC through various acculturation processes colonial power did emphasize to produce a new form of governmentality which would consist of docile, obedient, disciplined and question-less students. They would form an important core of modern citizenry. They had also diffused into indigenous society to instil such mode of thinking. By instilling appreciation of its fundamental principles of modern medicine and their bearing on daily conduct from the very beginning of school education and, also, forming a part of every accomplished native gentleman’s ordinary education, modern medicine and its techniques, medicine began to reconstitute the essence of traditional life.
It is highly noteworthy that Bramley’s (first founder principal of the CMC) feat until his premature death (19 January, 1837) to indoctrinate his students into strict code of moral, intellectual and habitual discipline smoothed the way for producing disciplined and docile modern citizenry. He wrote, “to educate natives so as to combine the communication of knowledge with the regulations of their minds and the directions of their habits of thought.” The students of the College had to go thorough different kinds of visual, verbal, auditory and psychic acculturations in their classroom teaching. They had also learned clock-time and moral acculturations in the shadow of European modernity.[114] Navya-Āyurveda unhesitatingly copied these characteristics in their own mold from modern medicine. Thus it also became a potent tool to produce modern citizenry for the colonial state and governance.
Consequently these neo-Āyurvedics, as Leslie argues, “have acted like their opponents who advocate reviving Āyurveda by utilizing modern science and technology: they have lobbied to influence governmental health policies…”[115] Thus the reconstruction of neo-Āyurveda was a definite entity in the consolidation of modern Indian state. In recent years neo-Āyurveda has again reinvigorated through AYUSH (Āyurveda, Yoga, Unani, Siddha and Homeopathy). It appears to be a new politics of health in India. Reddy envisioned it, “A scheme for producing midlevel primary care health workers, which many allopathic doctors oppose, will probably be implemented in states with severe physician shortages.”[116] State, medicine – both modern and traditional – and public health are mutually constitutive since 1835 in India. In this context, it may be benefitting to reproduce the observation – “The dominant form of ayurvedic education that developed from this background at the end of the nineteenth century was an integrated or a concurrent education system, which included both Ayurveda and modern medical subjects in varying proportions … The “biomedicalization” of Ayurveda is, however, not only a phenomenon that occurs within government institutions but also reaches into private practice…”[117]
[1] Michel Foucault, ‘The Crisis of Medicine or the Crisis of Antimedicine?’ Foucault Studies, 1, 2004, pp. 5-19. Quotation on p. 16.
[2] For a fuller study on the NMI and CMC and the genesis of hospital medicine in India see, Jayanta Bhattacharya, ‘The genesis of hospital medicine in India: The Calcutta Medical College (CMC) and the emergence of a new medical epistemology’, Indian Economic and Social History Review, 51(2), 2014, pp. 231-264.
[3] Joseph E. Di Bona, ‘Indigenous Virtue and Foreign Vice: Alternative Perspective on Colonial Education’, Comparative Education Review, 25(2), 1981, pp. 202-215. Quotation on p. 212.
[4] Ibid.
[5] Meer Ushraf Ali, ‘Treatment of Dysentery by Native Medicines’, Indian Medical Gazette, 3(1), 1868, pp: 83-84. Quotation on p. 83.
[6] ‘A Plea for Hakeems,” Indian Medical Gazette, 3(1), 1868, pp. 87-89. Quotation on p. 89.
[7] Eric Stokes, The English Utilitarians and India, Oxford University Press, London, 1959, p xiv.
[8] Ibid, 81.
[9] Ibid, xvi.
[10] Stephen Jacyna, ‘Medicine in transformation, 1800-1849’, in The Western Medical Tradition: 1800 to 2000, W. F. Bynum, Anne Hardy, Stephen Jacyna, Christopher Lawrence, E. M. (Tili) Tansey, Cambridge University Press, New York, 2006, 11-110.
[11] Ibid, 21.
[12] Ibid.
[13] Peary Chand Mittra, A Biographical Sketch of David Hare, W. Newman & Co., Calcutta, 1877, p. 138
[14] Ibid, pp. 138-139.
[15] The general accounts that Madhusudan Gupta was the first dissector, has been strongly contested. See, Jayanta Bhattacharya, ‘The first dissection controversy: the introduction to anatomical education in Bengal and British India’, Current Science 101.9, 2011, pp. 1227-1232.
[16] Pramatha Nath Bose, A History of Hindu Civilisation during British Rule, Vol. II, W. Newman & Co., 1894, Calcutta, p. 32.
[17] David Kopf, British Orientalism and the Bengal Renaissance: The Dynamics of Indian Modernization 1773-1835, Firma K. L. Mukhopadhyay, Calcutta, 1969, p. 143.
[18] Stokes, English Utilitarians, p. 43.
[19] Eric Stokes, ‘The First Century of British Colonial Rule in India: Social Revolution or Social Stagnation?’, Modern India, ed., Thomas R. Metcalf, Sterling Publishers Pvt. Ltd., New Delhi, 1992, pp. 173-198.
[20] John Rosselli, Lord William Bentinck: The Making of a Liberal Imperialist, University of California Press, Berkley, Los Angeles, 1974, p. 87. Also see, Demetrius C. Bougler, Lord William Bentinck, Clarendon Press, Oxford, 1892.
[21] Burton Stein, A History of India, Blackwell Publishing, Oxford, 2004), p. 220.
[22] Ibid, p. 221.
[23] Charles Maclean, Abstract of the East India Question: illustrating in a concrete manner the controversy between the East India Company and His Majesty’s ministers, J. Mawman, London, 1813, p. 3.
[24] Rosselli, William Bentinck, p. 187.
[25] C. A. Bayly, Indian society and the making of British Empire, Cambridge University Press, Cambridge, New York, 2002, p. 121.
[26] A. F. Salahuddin Ahmed, Social Ideas and Social Change in Bengal 1818-1835, Papyrus edition, Papyrus, Calcutta, 2003, p. 189.
[27] Rosselli, Bentinck, p. 185.
[28] The Works of Jeremy Bentham, ed. John Bowring, vol. 10, William Tatt, Edinburgh, 1843, p. 591.
[29] Rosselli, Bentinck, p. 85.
[30] Sumit Sarkar, Writing Social History, Oxford University Press, New Delhi, 2002, p. 309.
[31] C. A. Bayly, Empire and Information: Intelligence gathering and social communication in India, 1780-1870, Cambridge University Press, New Delhi, 2007, p. 265.
[32] The Correspondence of Lord William Cavendish Bentinck: Governor General of India 1828-1835, ed. C. H. Philips, in 2 volumes, vol. II, Oxford University Press, London, 1977, pp. 1279-1280. [Emphasis added]
[33] Ahmed, Social Ideas, p. 204.
[34] Erwin H. Ackerknecht, Medicine at the Paris Hospital, 1794-1848, Johns Hopkins Press, Baltimore, 1967, p. 15.
[35] Ibid, pp. 74-93.
[36] Ibid, p. 15.
[37] ‘Miscellaneous Critical Notices’, Calcutta Review, 13(25), 1850, p. xix. [Emphasis added]
[38] “Vernacular Education for Bengal,” Calcutta Review, 22(44), 1854, p. 328.
[39] ‘Sketch of an Indian Physician’, Lancet, 1, 1855, p. 48.
[40] S. Goodeve Chuckerbutty, Popular Lectures on Subjects of Indian Interest, Thomas S. Smith, Calcutta, 1870, p. 139.
[41] Robert Montgomery Martin, The History, Antiquities, Topography, and Statistics of Eastern India; Containing the Districts of Behar, Shahabad, Bhagalpoor, Goruckpoor, Dinajepoor, Puraniya, Rungpoor, and Assam, in 3 volumes, vol. II, Wm. H. Allen and Co., London, 1838, p. 106. [Emphasis added]
[42] Martin, ibid, vol. I, p. 137.
[43] Martin, ibid, vol. III, p. 142
[44] Ibid, p. 510.
[45] Martin, ibid, vol. I, p. 115.
[46] Ibid, p. 139.
[47] Ibid, p. 140.
[48] Whitelaw Ainslie, Materia Indica, vol. II, Longman, Orme, Brown, and Green, London, 1826, p. xxxiii.
[49] ‘Miscellaneous – Medical Advice’, Asiatic Journal 14(82), (October 1822, pp. 387-388 (387).
[50] Ibid.
[51] Ibid, p. 388.
[52] Ibid.
[53] Dominik Wujastyk, The Roots of Ayurveda: Selections from the Ayurvedic Classics, Penguin Books, New Delhi, 1998, p. 23.
[54] Calcutta Journal of Medicine VII (Nos. 10-12), 1874, p. 380.
[55] PC. Sen Gupta, ‘Soorjo Coomar Goodeve Chuckerbutty: The First Indian Contributor to Medical Science’, Medical History, 14(2), 1970, pp. 183-91.
[56] Report of the General Committee of Public Instruction for the Year 1836 (hereafter GCPI).
[57] GCPI, 1839.
[58] Gorman, ibid, p. 290.
[59] David Arnold, Toxic Histories: Poison and Pollution in Modern India, Cambridge University Press, New York, 2016, p.51.
[60] Ibid.
[61] Chuckerbutty, p. 82. Moreover, Chuckerbutty writes, “The Lieutenant Governor of Bengal has stated in his speech at the late distribution of Prizes to students of the Medical College, that he was firmly convinced that education was the surest means of securing the fidelity of the subjects to the Sovereign, and he quoted statistics to prove the truth of this doctrine as applied to India even in her present troubles.” – Ibid, 77.
[62] ‘Education of Native Doctors’, Asiatic Journal 22(127), 1826, pp. 111-121.
[63] ‘Sketch of an Indian Physician’, Lancet 65(1637), January 13, 1855, p. 48.
[64] Report of the Select Committee on Transportation; Together with the Minutes of Evidence, Appendix and Index, House of Lords, London, 1838, p. 196.
[65] W. J. Moore, Health in the Tropics or Sanitary Art Applied to Europeans in India, John Churchill, London, 1862, p. 6.
[66] For discussion at length on this issue see, Michael Adas, Machine as the Measure of Men: Science, Technology, and the Ideologies of Western Dominance, Cornell University Press, Ithaca, London, 1989, and M. N. Pearson, ‘The Thin Edge of the Wedge: Medical Relativities as a Paradigm of Early Modern Indo-European Relations’, Modern Asian Studies, 29(1), 1995, pp. 141-170.
[67] Whitelaw Ainslie, Materia Medica of Hindoostan, and Artisan’s and Agriculturist’s Nomenclature, Government Press, Madras, 1813.
[68] M. J. Bramley, ‘Introductory Address Delivered at the Opening of the Calcutta Medical College’, Calcutta Monthly Journal and General Register of Occurrences, Vol. II (Third Series), May 1836, pp. 1-7 (6). [Emphasis added]
[69] H. H. Goodeve, ‘Practice of Physic’, Calcutta Monthly Journal, ibid, pp. 19-26 (25). [Emphasis added]
[70] ‘Liberality of the Indian Government towards the Native Medical Institution’, Oriental Herald, 10(31), 1826, pp. 17–25.
[71] Centenary, p. 9.
[72] Minutes of Evidence taken before the Select Committee on the Affairs of the East India Company, I. Public, House of Commons, London, 1832, p. 448.
[73] ‘Native Medical Society’, Asiatic Journal, New Series, 7(26), 1832, pp. 84–85.
[74] Kopf, British Orientalism, pp. 183-184.
[75] Minutes of Evidence, ibid, 494.
[76] Brajendranath Bandyopdhyaya, কলিকাতা সংস্কৃত কলেজের ইতিহাস, প্রথম খণ্ডঃ ১৮২৮-১৮৫০, সংস্কৃত কলেজ, ১৯৪৮, p. 36.
[77] Adam’s Report on Vernacular Education in Bengal and Behar, Home Secretariat Press, Calcutta, 1868, p. 3.
[78] General Report on Public Instruction, 1844-45, Sanders and Cons, Calcutta, p. 98. [Hereafter GRPI]
[79] ‘Account of the Hospitals and Schools of Medicine in London’, Lancet vol. 37(944), October 01, 1841, pp.. 3-26.
[80] Charles Trevelyan, On Education of the People of India, Longman, Orme Brown Green and Longmans, London, 1838.
[81] GCPI, 1839.
[82] Rules and Regulations of Bengal Medical College, 1844, Government Press, Calcutta, 1844, p. 33.
[83] GCPI 1841, Appendix, No. VII, p. clxxiii.
[84] W. H. Sykes, ‘Statistics of the Government Charitable Dispensaries of India, chiefly in the Bengal and North-Western Provinces’, Journal of the Royal Statistical Society, 10(1), 1847, p. 3.
[85] Selections from Educational Records, Part II, 1840-1859, ed. J. A. Richey, Superintendent of Government Printing, Calcutta, 1923, 322.
[86] S. Anantha Pillai, Understanding Anaesthesia Jaypee Brothers Medical Publishers (P) Ltd., New Delhi, 2007, p. 13.
[87] GRPI 1851, p. 122.
[88] GRPI 1848, Appendix E, No. VIII, p. cli.
[89] Mel Groman, ‘Introduction of Western science into colonial India: role of the Calcutta Medical College’, Proceedings of the American Philosophical Society, 132(3), September, 1988, pp. 276-298.
[90] Sheldon Watts, ‘From Rapid Change to Stasis: Official Responses to Cholera in British-Ruled India and Egypt: 1860 to c. 1921’, Journal of World History, 12(2), Fall, 2001, pp. 321-374. Also see, William Campbell Maclean, Diseases of Tropical Climates, Lectures Delivered at the Army Medical School, Macmillan and Co., London, 1886, especially “Farewell Address”, pp. 329-337, and Jayanta Bhattacharya, মেডিক্যাল কলেজের ইতিহাস (২য় পর্ব), Pranati Prokashoni, Kolkata, 2023, especially chapter 10, pp. 182-201.
[91] Mark Harrison, Medicine in an Age of Commerce and Empire: Britain and its Tropical Colonies, Oxford University Press, Oxford, 2010, p. 291.
[92] G. Jan Meulenbeld, History of Indian Medical Literature, 5 volumes, 1A, Brill, Amsterdam, 2002, p. 2. This issue has been beautifully discussed in Introduction, pp. 1-6.
[93] Francis Zimmermann, The Jungle and the Aroma of Meats: An Ecological Theme in Hindu Medicine, Motilal Banarsidass, Delhi, 1999, 166. Also see, Rachel Berger, Ayurveda Made Modern: Political Histories of Indigenous Medicine in North India, 1900-1955, Palgrave Macmillan, Delhi, 2013.
[94] Surendranath Dsagupta, A History of Indian Philosophy, Vol. II, Motilal Banarsidass, Delhi, 1991, p. 433.
[95] Francis Zimmermann, The Conception of the Body in Ayurvedic Medicine, Ecole des Hautes Etudes en Sciences Sociales: http://philosophindia.fr/india/index.php?id=35 [ Accessed 6 August 2006] Also see, Zimmermann, ‘From Classic Texts to Learned Practice: Methodological Remarks on the Study of Indian Medicine’, Social Science and Medicine, 12(2B), 1978, pp. 97-103.
[96] “A Plea for Hakeems”, Indian Medical Gazette 1868, 3. (1): 87-90 (87).
[97] Ibid, 88.
[98] Girindranath Mukhopadhyaya, History of Indian Medicine: Containing Notices, Biographical and Bibliographical, of the Ayurvedic Physicians and their Works on Medicine, 2nd edition, 3 volumes, vol. 2, Oriental Books Reprint Corporation, 1974, pp. 14-15.
[99] Ibid, p. 17. That Madhusudan Gupta was the first dissector has been contested. See, Jayanta Bhattacharya, ‘The first dissection controversy: introduction to anatomical education in Bengal and British India’, Current Science, 101(9), 2011, pp. 1227-1232.
[100] Mukhopadhyaya, History of Indian Medicine, Volume 2, Introduction, pp.1-61 .
[101] Ibid, p. 22. [Emphasis added. All these characteristics reproduced from within Āyurveda remind the readers of the beginning of the CMC and the rise of hospital medicine in India]
[102] Ibid, p. 23. The mention of lantern slides leads us to believe the employment of modern technology, which is now developed in the form of power-point presentation (ppt).
[103] Ibid, p. 23.
[104] Ibid, pp. 23-24.
[105] Ibid, 24.
[106] Ibid, 25.
[107] Ibid.
[108] Ibid, 26.
[109] Ibid, p. 24.
[110] Ibid, pp. 24-25.
[111] Ibid, pp. 50-51.
[112] Ibid, p. 31. [Italics added]
[113] Ibid, p. 77.
[114] For a full-length discussion on this issue see, Jayanta Bhattacharya, মেডিক্যাল কলেজের ইতিহাস (১৮২২-১৮৬০), প্রথম পর্ব, প্রণতি প্রকাশনী, কলকাতা, ২০২২ (History of the Medical College – 1822-1860, 1st part, 2022). Otherwise, one may like to consult Report of the General Committee of Public Instruction of the Presidency of Fort William in Bengal, for the year 1836 (abbreviated as GCPI 1836), pp. 31-67.
[115] Charles Leslie, ‘The Ambiguities of Medical Revivalism in Modern India’, Asian Medical Systems: A Comparative Study, ed. Charles Leslie, Motilal Banarsidass, Delhi, 1998, pp. 356-367, quotation on 358.
[116] K. Srinath Reddy, ‘India’s Aspirations for Universal Health Coverage’, New England Journal of Medicine 373(1), 2015, pp. 1-5. Quotation on p. 4.
[117] Dagmar Wujastyk and Frederick M. Smith, ed., Modern and global Ayurveda: pluralism and paradigms, State University of New York, New York, 2008, pp. 7-8.








তথ্যসমৃদ্ধ লেখা, এত বড় ইতিহাস সংক্ষেপে তুলে ধরার জন্য অসংখ্য ধন্যাদ , সমৃদ্ধ হলাম
Thank you. Learnt a lot. Interesting that the tensions you highlight still persist.
লেখাটি খুব ভালো হয়েছে।…. না, ইতিপূর্বে এই নিয়ে কোনও লেখা বাংলা/ইংরেজি/ হিন্দিতে পড়িনি।( আজকাল অন্য ভারতীয় ভাষার লেখা গুলোও বেশ তাড়াতাড়ি হিন্দি অনুবাদে পাওয়া যায়)
অনেক ধন্যবাদ দাদা। লেখাটির খুব দরকার ছিলো। … আমি নিজে যেহেতু CMC prescribed teachings ছাড়াও প্রায় “টোল” System এই আলাদা করে পড়েছি ( teachers being CMC Senior Profs … সবচেয়ে close এবং যিনি আমাকে প্রায় constant teaching and guidance দিয়েছেন… Dr.M.N Sarkar.. he wanted to impart his life acquired knowledge… তাঁর কাছে এবং তাঁর বন্ধুদের কাছ থেকে didactic পড়াটা পেয়েছিলাম … with minimum extra effort from my part! ..😊)….Dr.MN Sarkar enjoyed a long life (91+) তাই all throughout my School and College life, he was my main guide. উনি এই teachings গুলো বেশি details এ দিতে পারতেন, কারণ, he was the best Sanskrit Speaker amongst his colleagues এবং যেহেতু “ফার্সী” ও শিখেছিলেন, সেহেতু Unani traditions গুলোও সুন্দর analysis করতে পারতেন।…. আমি ওঁর কাছে থেকেই ঐ Unani traditions গুলো জেনেছিলাম। ভারতে যখন প্রথম All India Radio সংস্কৃত সম্প্রসার শুরু করে, তখন উনি এই basic Ayurveda traditions গুলো ( যেমন আপনি লিখেছেন — with the view of Navya Ayurveda) সংস্কৃত ভাষায় ছোটো ছোটো talks দিতেন। বেশ interesting হতো সেগুলো।
আপনার লেখা পড়ে এগুলো মনে পড়ে গেলো। 😊
আমার নিজের প্রতিটি patient ই booked and registered….. আমি pt profiling এ এই Principles গুলো incorporate করেছি। …. আমার registers যারা যারা, ডাক্তাররা দেখেছেন (pt রা তো বটেই) তারা জানেন। আপনাকে দেখাবারও ইচ্ছা রইলো। 😊
Thanks to Dr Jayanta Bhattacharya for posting this rich article in this platform already established for those who are interested in research works.
This article is so rich because it tells us the history of not only learning and practicing of British medical education in India but also change of complexion of Ayurveda as well as Hekimi medicine till formation of AYUSH in modern India in the National Health Policy as a substitute to allopathic medicine for those who like to avail themselves of the system.
The references used in the article are all celebrated ones. Wonderful write-up to know the history has been presented by Dr Jayanta. Thank you, again.
A great write up Jayanta. Very fascinating. What a big effort it must have been for you to gather and research in to all the info. Many thanks for enlightening us with your hard work. Congratulations. 😀
So good👍