

The Pandemic
State had known at the very onset of pandemic that the extra covid patients (over existing non-covid ones) could not be accommodated within such prevailing scarcity of hospital beds and trained human resources. The State in response at the start tried to give a false impression of having low burden of cases by restricting covid-19 testing. But in due time, public criticism in urban areas forced open the criteria of testing. This resulted in sudden spike in detection of positive cases (limited to urban areas) which overwhelmed the existing healthcare facilities in no time. It was an expected fallout of the initial failure of State to test for Covid-19 in adequate numbers as the lockdown failed to contain the spread of virus in the community. But the rural areas still remain at the mercy of fate and is on the verge of a human disaster in the making.
Bottom line remains that the ‘quantity’ of hospital beds providing ‘quality’ healthcare in a system guided by free-market dynamics depends on the ability of the invested capital to make profit, and does not take into account the actual requirement of the society as a whole. That means the ‘quality’ of service available in even big private sector which caters to the middle class and the rich (i.e. top 10%) is not homogeneous, but goes down in accordance to the extent of affordability. Based on this logic, any expansion of private healthcare facilities to accommodate such extra covid patients looks bleak because of current economic slowdown which dampens the future prospects of profit.
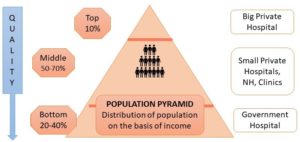
Meanwhile, the State continues to manoeuvre majority poFigure 4: Population pyramid (based on distribution of income) suggests that 60-80% of population is dependent on private health sector and quality of treatment decreases in accordance to affordabilityor (bottom 90%) covid and non-covid patients within the existing premises of suboptimal treatment in either small private settings or public hospitals. On the other hand, such available healthcare resources are utilized for mostly asymptomatic patients (as an alternative to home isolation) or for mildly symptomatic covid-19 patients just requiring oxygen therapy. The rest few covid-19 patients requiring hospitalization and state of art respiratory support facilities are left with no option because such facilities are very few in number, restricted to State-run tertiary care facilities, often manned by untrained human resources. Rationing of ‘quality’ private health care facilities for such advanced care is being done for just the ‘select few’, leaving the rest ‘majority’ at the mercy of fate. [1] Still the total around 20,000 ventilators available in India at present, mostly limited to private sector falls short of the estimated 110,000 – 220,000 ventilators statistically required to cater the total population. The State in response has avoided testing such potential sick patients in adequate numbers. The continuing lockdown is used as a measure to help restrict transfer of such sick patients from periphery to major cities to avail tertiary care facilities. Rest eligible lucky few who get access to State-run hospitals are exposed to sub-optimal treatment in State-run ICUs with resultant higher death rates.
Overall, this is supposed to create a false impression that the State is doing the best to serve the ‘poor majority’. Recent purchase of another 60,000 ventilators by the Central government to bridge the gap hoisted over the last three decades in providing advanced treatment in State-run hospitals have simplistically overlooked the obvious lack of trained human resources to manage them. Converting premier educational institutions like Medical College, Kolkata (MCK), and Sagar Dutta Medical college into dedicated covid-19 hospital for such predominant mild to moderate cases, without upgrading them for advance life support is one such glaring example of populist measure. Recent protests by junior doctors in MCK have successfully highlighted such plight of poor patients caused by under-utilization of the available resources in dealing with both covid and non-covid patients. The success of such short-sighted and ill-managed State modus-operandi to pacify the common-man will depend on the same ignorance. Majority of them being poor and illiterate, are divided on political loyalties based on more important agenda of ensuring food security and staying alive, especially during this economic lockdown. The doctors who are the fighting the pandemic in turn feel helpless and dejected, being forced to work under extreme stressful conditions and still unable to provide required treatment due to either lack of proper infrastructure or proper training.
(to be continued)
[1] Brooking report









