

Preliminary Cues
In the last chapter, how modern public health programs in India through the deployment of CMC graduates to different dispensaries across the Northern, North-Western and Bengal provinces was detailed. Briefly speaking, the journey can be represented in a sketchy way like this – CMC (>) Dispensaries (>) Inception of Public Health. This is substantiated by dispensary reports compiled in 1847. Through dispensaries Western medicine penetrated to the remotest parts of India and people were attracted towards it. To be sure, there were also some problems to give access to all the people asking for relief –
The room for the distribution of medicine, and the space for seats of out-patients, are also so small, that if even one-third of the average daily applicants enter the Dispensary at once, half of them are obliged to stand. This is the only reason why the respectable people hesitate to come in the Dispensary for medicine, where they are very justly apprehend the disagreeable necessity to of either standing up till they are called, or to sit down with persons whose touch, nay, even proximity, is not only calculated to cause a disgrace, but to impose upon them the necessity of washing their body after such a contact has taken place, even if it be so by chance.[1]
Such an image of government hospitals is glaringly true even in the today’s India even after about 180 years since the beginning of the dispensaries. But this description indicates that the demand among Indian population for western treatment and medicine was steadily increasing. The Report further proceeds –
The people of Upper Hindoostan are still strongly prejudiced against female freedom and female happiness, that they always take the best care to keep their wives and daughters in the innermost recess of their cooped-up houses; they have no faith on each other, and consequently none of the other sex, but such as belong to the family, can have an access to the family part … the physician is permitted to feel the pulse, by which guide alone they must be treated. It is no wonder then that for the diseases of the urinary and generative organs they should invariably have recourse to nurses and old grandmothers … The Hakeems have no medicines to expedite delivery, neither do the people approve of the plan of administering medicines to pregnant women.[2]
It is quite interesting to note such a description of the inside of the Indian families that in the dispensary reports. It can also be seen as a ‘modernizing’ project of colonial governmentality, where doctors served as “information gatherers”. According to Bayly, “Physicians were, in addition, important information gatherers for the state.”[3] Those who resided in cities held regular councils and could frame broad calculations of mortality rates by ordering the custodians at the city gates. Thus the profession of medicine as a whole and individual medical person were quite intimately tied up with the emergence of modern Indian state. Dipesh Chakrabarty draws our attention to the intricacies of this move from an altogether different perspective –
The question of health, in turn, reflected the relations of power under colonial rule, the idiom of gender (the imperial theme of the emasculation of the colonized) in which it was often manifested, and the extent to which the male body itself had become a signifier for these relationships … The critical in all this was to reform women, for these arrangements could not be put in place until women were educated in the new rules of the body.[4]
Chakrabarty’s analysis adds new dimension and tools of analysis to the dispensary regarding family/private space of women and inaccessibility to male doctors inside the space. But it also points to the fact, as Bayly has analyzed, that through dispensary reports colonial authority was also gathering information regarding applicability of new techniques for the making of new ‘citizenry’ for the emerging and nascent semi-modern state.

Regarding administration and daily practices of dispensaries throughout India, there were differences between the way Bengal adopted for the functioning of dispensaries and the practices adopted in Madras and Bombay for dispensary functioning. The colonial authority was not much sure about similar results as accrued from the experience of Bengal. On December 8, 1841, a government circular stated – “We sanction the formation of Dispensaries in the towns of Trichinopoly, Madura, Masulipatam, Nellore, Bellary, and Cadappa, as an experimental measure … but we desire that no others may be established, until we are informed of the expense, and are satisfied with the results of those now sanctioned.”[5] It was further elaborated that “Dispensaries subsequently authorized” were “One on the south side of Madras, for the benefit of the poorer classes of the inhabitants of Triplicane, Royapettah, St. Thome, and the adjoining villages; also at Salem, Calicut, Vizagapatanam. And Kurnaul”[6]
Moreover,
In Bombay the Dispensaries are under the European medical officers, and not, as in Bengal, under a sub-assistant surgeon. The judge and magistrates to allot a public building, or to hire one. Not indiscriminately open to every patient. The Native, inhabitants with the ordinary diseases not to be admitted as in-patients, but accessible for advice and medicine to all out-patients … Each Dispensary to have ten barrack-cots, matrasses (sic), pillows, and twenty quilts. Each to have a second dresser or assistant. To be inspected by the magistrates and superintending surgeons. When females apply, a separate ward to be allotted to them.[7]
What is important here is that despite differences in approach to exactly how medical help will reach common people, the moot question was addressed in all the cases, be it Bengal, Madras or Bombay – Western medical help and aid to the poorest people of India or public health. In case Bengal, the centre of production of medical personnel was CMC, the conduits were dispensaries. What was reached at was public health. In other two instances of Madras and Bombay, the issue was fully taken up by European doctors only. It might have limited the scope of expansion of public health in Madras and Bombay.
This is further substantiated by Surgeon-Major Thomas Farqhar of Bengal Medical Service, “within the last thirty years the dispensaries in India, which in 1840-42 numbered twenty-two – that is, in Bengal 14, and in Madras 8 (there is no such early report from Bombay available) – have gradually increased year by year till they are returned for the year 1867-8 as amounting to an aggregate of 493 – that is, for Bengal 425, and in Madras 68.”[8] He proceeds further, “As might be expected, the number of sick reported as at tending these numerous institutions has greatly increased also. Thus they were, for Madras and Bengal,
In 1841-2: In-door patients – 3, 693
Out-door patients – 95,573
In 1867-68:
In-door patients – 83,013
Out-door patients – 1,787,743.
And for Bombay – 305,170”[9].
Finally, Farqhar concluded, “Politically speaking, the benefits yearly experienced by about 2,000,000 of the people of India from institutions of this benevolent character, established and supported by the English Government, must be of no small importance in retaining the good will of the people.”[10]
Annual Reports of the CMC
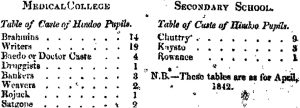
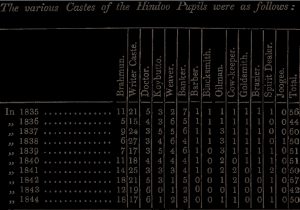
Interestingly, at the very beginning of the report for 1841-42 caste distribution of the students was specifically mentioned. It leads us to ponder over the fact that though Western medical system was secular in general terms in its core the millennial, traditional caste system was registered in its actual practice. From present day’s Derridean analysis of deconstruction theory it definitely signifies an aporia – a Greek term denoting a logical contradiction, ‘aporia’ is used by Derrida to refer to what he often calls the ‘blind spots’ of any metaphysical argument.[11] Though I am not a ‘deconstructionist’ nor I am dealing my paper or analysis from Derridean perspective at all, this particular term may be useful to understand the hiatus between avowed secular nature of education and non-secular caste pattern getting its place in the annual reports of the CMC.
The College report represents caste distribution of students in the following way.
Annual examination of 1840 continued for 10 days. Finally, the following 7 students were credited with “letters testimonial of the Medical College.” These students are – Madhusudan Gupta, Jadab Chandra Dharral, Chummun Lal, Rajkisto Chatterjee, Gobinda Chandra Gupta, C. T. Imlay, and Navakrishna Gupta.[12]
In this session’s report there were definite proposals on revamping of lectures on midwifery, chemistry (where few lectures on medico-legal medicine, precursor to today’s forensic medicine, were to be included), materia medica, botany and practical anatomy. Then came the provision for the clinical clerk who would “remain on attendance on the Hospital during night … That one of the Clerks should remain at night by turns.”[13] To note, “In regard to Medico-legal Instruction Dr. O’Shaughnessy reported, that from the time of appointment as Professor, he had always given several lectures on Toxicology (one of the most important branches of Medical Jurisprudence) in each of his courses, and that in 1840, he had given six lectures of this kind.”[14] The annual examination consisted – (1) “In all the Candidates answering several medical questions in writing without any assistance, &c. (2) In an Oral Examination.”[15] Many changes occurred in 1841. After David Hare, Dr. W. B. O’Shaughnessy took the charge as secretary of the College. And Dr. O’Shaughnessy, after a few months, departed for Europe. There was improvement of the dieting of of patients in the Hospital.[16]
There is an interesting report regarding students’ irregularities in attendance in classes, dissection and hospital duties etc. But on further scrutiny it became evident that “many of the lads lived a great distance from the College (in several cases six miles, and in one eight) and having no means in their village of ascertaining the exact time, were oftener after than before the time appointed calling the roll, and were consequently reported absent, although they in fact in the College during the day specified, and attending to their duties … walking to and fro so many miles every day in the pursuit of knowledge…”[17] It was noted by the College Council and “to protect the really industrious and meritorious students from the bad impression … the system of calling the roll had been somewhat modified.”[18]
From this small description it transpires that (1) clock-time acculturation practised in the College was not at all relevant for a good number of students residing at great distance from it (supposedly villages), and (2) seemingly, the then Calcutta had contained within it a number of ‘Calcuttas’, all were eventually engulfed into the new urban code of everyday life consistent with the emerging techniques of producing a ‘new’ kind of citizenry, and (3) the introduction of clock-time was an important tool in this regard. It points to the fact that colonial power through its governance made the ‘power’ dispersed, not centralized, throughout the indigenous society. The political order is maintained through the production of “docile bodies” – passive, subjugated, and productive individuals. Through its many institutions – schools, hospitals, prisons, the family – the state brings all aspects of life under its controlling gaze. The institutional disciplining, surveillance, and punishment of the body creates bodies that are habituated to external regulation, centred on the body as a machine: “its disciplining, the optimization of its capabilities, the extortion of its forces, the parallel increase of usefulness and its docility, its integration into systems of efficient and economic controls … an anatomo-politics of the human body.”[19] And thus produce the types of bodies that society requires.
Coming back to the Report, students were trained to have “ready skill absolutely required, to ensure the successful Surgical treatment of diseases … The mode of appointing Dressers, the distribution of duty among them, and the performance of operations by the students themselves, combined with the Clinical Lectures delivered on the cases”[20] were very productive. Similar patterns were pursued in case medical cases. But what is glaringly absent in these detailed accounts is the mention of any laboratory activities, which were started by W. B. O’Shaughnessy 5 years back.
In case of Materia Medica, under the professorship of Dr. F. J. Mouat, a system of “arrangement, classification, and method of instruction had however been adopted, as nearly as circumstances would permit, on the plan pursued in the course of Professor Christison of Edinburgh.”[21] In the Secondary or Vernacular Class, sub-assistant surgeons Nava Krishna Gupta and Shibchandra Karmakar – two Indians – were appointed as teachers.[22] Indians began to be gradually elevated to rank of teachers at the CMC. In memory of W. B. O’Shaughnessy’s contribution to the College and the Asiatic Society, a rigorous examination of chemistry was held among students. The most creditable essay was signed with motto “Nil Desperandum”, the second was signed “Ex nihilo nihil fit”, and the third one was signed “If ignorance, be bliss, ‘its folly to be wise.”[23]
Prasanna Kumar Mitra was appointed as Resident Surgeon, Midwifery Hospital. He also received Dr. Goodeve’s Midwifery Scholarship OF 16 Rs. Per month. Additionally, as Resident Surgeon, he had drawn a salary of Rs.50 per month.[24]
There was a detailed report on “Dispensaries superintended by Ex-Students of the Medical College”. According to this report, “Bhowanipore – Sub-Assistant Surgeon Kallachand dey”, “Pooree – Sub-Assistant Surgeon Nilmoney Dutt”, “Moorshedabad – Panchanan Sreemony”, “Dacca – Nabinchandra Paul”, “Chittagong – Rajkristo Chatterjee”, “Putna – Rameswar Awasthee”, “Benares – Ishanchandra Ganguly”, “Cawnpore – Ramnarain Doss”, “Allahabad – Jadabchandra Dhara”, “Agra – Umacharan Sett”, “Bareilly – Jadab Chandra Seth”, “Delhe – Chummun Lall”, and “Jubulpore – Shyamacharan Dutt”[25]. From this report, it appears there was Bengali infiltration and, subsequent Bengali colonization, into different parts of colonial India through dispensaries and, presumably, through other administrative services.
Report on the Reforms of the CMC
In his letter to G. A. Bushby, Secretary to Government, General Department, on 17 July, 1841, T. A. Wise, Secretary, General Committee of Public Instruction, wrote at length about how to improve general status of education at CMC and make it more modern compatible with at least the provincial schools of medical education in Europe. Wise wrote, “its defects, however, are sufficiently obvious, seeing that whatever short-comings might become observable, no individual had the power of modifying them…”[26] So the question of overhauling the system itself came to importance. He carefully mentioned, “In its importance to the Native population, not only as a Hospital, but as a School of instruction, the probable benefits of Midwifery practice and Courses of Lectures cannot be too highly esteemed … qualifying themselves to become Nurses and Midwives in the community, and thus be saving much of the human life … It would also afford livelihood to persons so instructed…”[27]
In the above-mentioned letter of T. A. Wise it was specifically mentioned – “The night residence of the Clinical Clerks has been duly provided for in quarters lately occupied by Ceylon students.”[28] The “Printed Rules of the Clinical Clerks and Assistants of the Hospital” clearly stated that “the eighteen senior Students will each in turn, for one day, take the night duties of the Hospital being provided with a room and lights.”[29] Another important development is produced below.[30]
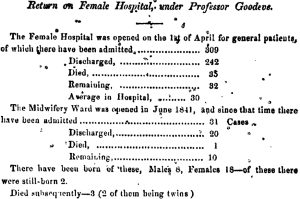
Interestingly, it was noted that the “Women admitted into the Midwifery Hospital are, at present, of a very inferior class, chiefly Hindoos and Mohamedans … one respectable European Female has entered the wards and been safely delivered; she was lodged in a separate room, and secluded from the visits of pupils.”[31] The question of race looms large in this reporting – the respectable European lady is lodged separately and not allowed to be examined by Indian students of the CMC. Again, the question of aporia can be remembered – to understand the hiatus between avowed secular nature of education and non-secular race superiority getting its place in the management of Indian and European patients. This European patient and others of similar race who were admitted into the hospital expressed “themselves of well pleased with the arrangements, and have promised to recommend others to our charge.”[32]
The establishment consisted of a European nurse, 2 native nurses, 2 ward coolies and 5 other servants (“Bheestie, Sweepers and Cooks”). Moreover, “the mortality of parturient women amongst the native population, unaided by European science is nearly 20 per cent, that of the children greater.” But under European doctors’ supervision “the mortality has hitherto averaged less than 3 per cent.”[33]
Goodeve reported that the hospital was established “in opposition to the very strongest prejudices of Asiatics of all classes, that it has existed little more than six months, and that it has already received within its walls a number of patients, mostly equal the average delivered during the same period in the Westminster Lying-in Hospital.”[34] It reveals quite clearly that due to huge population in India the number of delivery at the midwifery hospital of the CMC averaged that of the first-rated hospital like Westminster Lying-in Hospital. So the students of the CMC had more than ample opportunities to learn about new diseases and their management from vast, heterogeneous and diverse Indian population coming at the CMC for medical and surgical relief, and, to add, female diseases too.
Moreover, the “first course of Midwifery Lectures was delivered during the last hot weather (must be the summer of 1841), it was attended by all the senior Students, and several of those who had already passed their final examination. The whole subject of Parturition, with the history and treatment of the ordinary Diseases of women and children, were embraced in this course of Lectures … Within the last few weeks, three Female pupils, European and Eurasian, have entered, and are very anxious for knowledge.”[35]
To mention, in 1844 Goodeve wrote a book Hints for the general management of children in India in the absence of professional advice which was published from Calcutta. The book had seen many editions and, though the discipline of paediatrics was not in the offing, the book proved to be very useful for students and practitioners in India. In the original edition of 1844 Goodeve made it clear in his Preface –
In offering these few pages to my patients, I do not, for a moment, pretend to give them a complete treatise on children’s diseases. Nor do I wish, in any way, to prevent their taking medical advice, where it can he obtained. On the contrary, I would earnestly caution them never to trust to their own judgment, when they can procure professional assistance. The observations and advice contained in this little pamphlet, are intended, merely to aid those (a large class in India) who are placed at a distance from the advice of medical practitioners, and if this work prove beneficial in a single case, I shall be amply repaid for the time I have bestowed upon the subject.[36]
In the “Preface to the Third Edition” from London, October 1852, he wrote –
When I published the Second Edition of this book in 1844, a few months before I retired altogether from professional life, I had reason to suppose that long ere this time it would have been superseded by some more efficient work of the kind. This I understand has not occurred, and whilst the former editions are out of print, a demand for the book itself continues. Some spurious copies having in consequence been produced in the meantime, I have complied with my Publishers’ request to bring out another, and I hope an amended edition of my own.[37]

(Goodeve, in the middle, in a group photo with family and friends in England – undated)
T. A .Wise’s (Secretary. GCPI) letter to government on 17 July, 1841, contained final recommendations as – (1) “A new Operating Room’, (2) “Cots and Bpxes for the Secondary Class Students, and Venetians to the western door”, (3) “The appointment of Mr. Webb as Curator, (4) “The advance of Rupees 300 to the College Council for the purchase of professional books as Auction, when favourable opportunities occur”, and (5) “Samples of Materia Medica from H. C. Dispendary on an Indent from the Professor of Materia Medica.”[38] What is glaringly absent in these recommendations is the need to carry forward any laboratory activities.
It will be further substantiated from next proposals – “a Lecture should be given once a week, by Professors of Medicine and Surgery, on any of the important diseases of the Hospital. To the Lectures on Midwifery, it was agreed that those on the Diseases of women and children should be added.”[39] On “System of Lecturing” it was mentioned – “The Lectures on Physiology and on Materia Medica, and Therapeutics being of the greatest importance to the Student … 100 Lectures should be given every year by the Professor of Anatomy, and Physiology … thirty Lectures should be delivered each year on Midwifery and the Diseases of women and children … Lectures on principles of Chemistry should be diminished to thirty, and those on Materia Medica be increased to one hundred, with a few Lectures in each year on Medico-legal questions”[40].
To note, in the “Speech of the Right Hon’ble the Earl of Auckland, at the Medical College, February 10th, 1842”, it was mentioned – “he looked on this College as the most important and the most interesting of all the Institutions which had been founded by the Government for purposes of education … and the happy results of the instruction imparted at it would be felt and acknowledged even beyond the limits of our own Empire.”[41] Such was importance of the CMC to the highest colonial authority. But little was done towards the end of making a genre of new researchers and scientists.
In the Annual Report for the Session 1842-43, it was jubilantly noted –
the Sub-Assistant Surgeons, educated in the College, perform their duties, and the amount of good which had resulted from their exertions … the intrinsic value of the Dispensaries, which are so well adapted by their internal economy to obtain the confidence of the native inhabitants … Many have their sight restored, others have been cured of hydrocele … relief from the successful operation for “stone in the bladder” … saved from a miserable death by the amputation of diseased members, and the large tumors have been removed … Country medicine at each of these Institutions appear to have been generally used…[42]
Many alterations were made in the buildings of the College to extend its usefulness. Moreover, “the pupils from being located without the walls, not being sufficiently under the control and personal superintendence of the college authorities, it has been determined by the Government … to remodel the plan of the premises.”[43] It is intriguing to note that a kind of Panoption, as discussed earlier, was in operation to keep the students under full-scale surveillance of the College administration. Moreover, the new discipline required for the emerging and disciplined, docile citizenry out of the CMC students was also breeding and doing its job. The “inside” of the College was different from the “outside” of local inhabitants who were not brought under the umbrella of this strict code of daily living.
The Report continued – “The new structures will all be enclosed within the walls of the college compound, for which purpose the Civil Architect has been directed to negotiate for the purchase of certain adjacent huts, and portions of ground and roadway…”[44] The breeding ground of the new disciplinary governance and ‘modernity’ was expanding its territory.
The new system of calling the roll was introduced along with “granting of the Circlets of Merit”.[45] Auckland, before his departure from Calcutta, bestowed two handsome compound microscopes – one was of greater value, the other of lesser one. Satkari Dutta, after a searching trial of public examination, was awarded the first one, while Prasannakumar Mitra was given the second one.
Notably, Ramkamal Sen, Dewan of the Bank of Bengal, donated a gold medal at the disposal of the College Council and Rustomji Cowasjee, Esq. of Calcutta, “in the most handsome manner placed at the disposal of a sum of Company’s Rupees 600, to be devoted annually to the purchase of a Gold Medal, for the most student in practical Anatomy. Most importantly, a compulsory deposit of “two Rupees from each dissecting student” was put into effect.[46] The initial anxiety about the first dissection was publicly made redundant and new bold steps were being gradually taken by the College Council because of the fact that the CMC had already etched out its permanence in Indian society.
The Midwifery ward, according to the Report, continued to prosper and “was always full patients, and presented to the students a variety of instructive cases, amongst women of all religions and nations.”[47] Prasannakumar Mitra was the resident surgeon of the female or obstetric hospital. “Raja Kissennath Roy presented to the funds of the Hospital a munificent donation of Rupees 700.”[48]
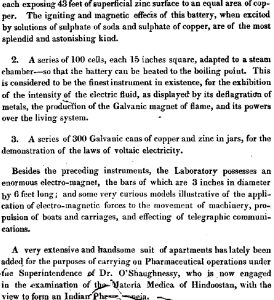
From all these accounts of donation in cash or kind from Indian rich people, it transpires that though the British had founded the CMC its development and survival depended to a large extent on Indian elites. Even at its beginning, when laboratory activities were in its heydays under the mentorship of Dr. W. B. O’Shaughnessy, we find such report that “a magnificent series of Galvanic batteries presented to the College by public subscription”[49]. Below are descriptions of laboratory performances in 1837-38.[50] Ruefully enough, in the annual reports of succeeding years there is no mention or trace of laboratory works done in CMC.
The attraction of this institution’s teaching and classes were so much alluring that “Baboo Doorgachurn Bonerjee, late Head Master of Mr. Hare’s School, and Ganindramohan Tagore, a distinguished pupil, and scholar of the Hindoo College, and son of Baboo Prosonnokumar Tagore, together with the Apothecary to the general Hospital, were attending the lectures delivered in the College, as amateurs … and the branches of science taught within its walls, are beginning to be held among the native community … who have not enjoyed the benefit of a professional education in Europe…”[51]
There were also reports of students’ unrest of the Secondary or Military School attached to the CMC and certain irregularities were committed in the neighbourhood by the students, due to which “after careful examination of the offenders, ten were recommended to Government for expulsion”[52].
As an aside, it may be important to cite that Emma Roberts, an English traveller, came to Calcutta in 1830s. Her article was published in Parbury’s Oriental Herald. She observed – “no small number turn the experience which they have acquired in India, to good account at home, the greater proportion who have distinguished themselves are indebted to their superior attainments in branches of science independent of their professional studies.”[53] She intended to offer her observations “to those gentlemen who look into India as a field for the pursuit of their professional career”[54]. She also commented – “as I am informed upon the best authority, that the Brahmin and Hindoo youths amongst these medical students, have so completely overcome their prejudices as to the study of anatomy from dead subjects by dissection, with as much ardour as any pupil of London hospital”[55].
It is intriguing to note that the act of dissection by the students of the CMC was much lauded, but their original researches in medical science were almost nonexistent in various accounts.
A few examples may elucidate the issue in a proper way. H. H. Goodeve, in his lectures in 1848, remarked, “in less than two years from the foundation of the college, practical anatomy has completely become a portion of the necessary studies of the Hindu medical students as amongst their brethren in Europe and America. The practice of dissection has since advanced so rapidly that the magnificent rooms erected four years since, in which upwards of 500 bodies were dissected and operated upon in the course of last year, now amounting to upwards of 250 youths of all…religions, and castes…as the more homogeneous frequenters of an European school.”[56]
Another account reads thus, “it appears that the number of native students attending the surgical class amounted to 3,952, out of which great number 3,589 were present at all the lectures during the season; in the anatomical and physiological class 3,844 entered, out of which 3,430 attended every lecture… from the month of November, 1846, to that of March, 1847, being a period of only five months, nearly 500 bodies had been dissected by the native students; – an astonishing number, when the prejudice to be overcome is considered…”[57] Think of the scenario!
In Ruth Richardson’s (the celebrated author of the book Death, Dissection and the Destitute) estimate, bodies taken under the Anatomy Act (the first ten years from 1832-33 to 1841-42) for London hospitals only are – 135, 141, 194, 206, 184, 209, 156, 168, 178, and 110 respectively. Difference between the numbers of dissection in Calcutta and London was quite phenomenal.[58]
Coming back to the Reports discussed so far, “judicious alterations (suggested by increased experience in teaching the foundation of all Medical and Surgical Science) have invariably been adopted to render the course of instruction more complete and perfect.”[59] In the class of surgery under Raleigh “The mode of appointing Dressers, the distribution of duty among them, and the performance of operations by the students themselves” etc. all were brought into operation.[60] In the classes of Practical Anatomy, Richard O’Shaughnessy commented – “in this respect some of them (students) were equal to any students of their standing in the best European Schools.”[61]
In the “Class of Medicine”, “Each Clinical Clerk was required to interrogate and examine the patient on his admission, to exercise him in the framing correct and accurate diagnoses of disease … This being very nearly, if not identical with, the system pursued in the celebrated Ecoles Cliniques of Paris and Strasburgh, which received the sanction of some of the most eminent Physicians in Europe.”[62]
It may be interesting to note from the above statement that the CMC, increasingly modeled on the UCL, was making its syllabus, unlike UCL, more dependent on the French system which laid more emphasis on pathological anatomy and clinical learning than on laboratory activities. The UCL tried in the 1830s to join the theoretical study of science to the practical work of the clinic, as was already underway in Germany. But there was resistance from the more orthodox section of society – “Likewise in Britain, when the new University of London tried in the 1830s to join the theoretical study of science to the practical work of the clinic, as was done in Germany, the hospital teachers at St. Bartholomew’s objected strenuously that the new school was superior “in no respect” and that it was “much inferior” to others in its practical instruction.”[63] But we shall see later that the German experience was referred to while proposing for residential education at the CMC.
For surgical cases, “of the deaths, 28 occurred in from 2 to 7 days – 12 from 7 to 14 – 4 from 14 to 20 – and 2 from 20 to 40 days.” And 163 European fatal cases died within forty-eight hours after their admission into the Hospital.[64] Regarding W. B. O’Shaughnessy’s contribution for the College, it was reported – “The subject of Chemistry was taught during the past years by the late Professor Dr. Wm. O’Shaughnessy, now in Europe, whose merits and distinguished talents the Government has so often recognized.”[65] Though his “merits and distinguished talents” were recognized, but his zeal for original researches, laboratory-based hands on training and free thinking for science were not pursued at all. It may be safely said that there was a stasis in laboratory-centred scientific practices.
All the departments and buildings were renovated and sometimes new buildings were rebuilt during the year – “In addition to the departments above enumerated there are, an out door Dispensary, Dead houses, Cooking rooms, Stables, and Lodges for the durwans and the sepoy guard … The College originally formed the Petty Court jail of Calcutta, and all subsequent additions to it have been made at the expense of Government in the Education Department.”[66] In this concluding remark of the Report all types of donations from Indians – in cash or in kind – were just erased from the record.
Report of the 1844-45 Session
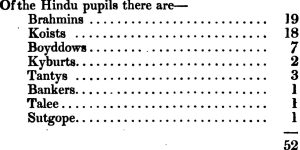
At the very beginning of the Report caste distribution of the 1st year class is detailed – of “the Hindu pupils, 4 are Brahmins, 5 … Kaists, 2 … Chuttrys (most likely carpenter/weaver caste, 4 … Rowanees (difficult to understand now, may be belonging to agriculturalist caste).”[67] Later, in the Report, it was more elaborately described.[68]
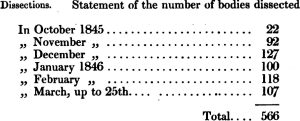
The recurring theme appeared even in Report of 1845-46 session.[69]
Let us compare now the number of bodies in the single session 1845-46[70] to the bodies dissected in London over a 10-year period. The figure is simply astounding!
Number of bodies dissected at London hospitals can be had from following table.[71]
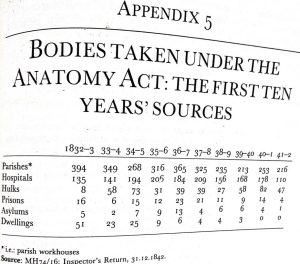
Any interested reader should ask: where did such huge number of dead bodies come from? We have a few plausible answers. In 1851, the number of bodies dissected was 722 – an increase of number by 100 from the previous year.[72] Buckland noted that a large proportion of the corpses, instead of being burnt, were either thrown into the river, or consigned for dissection to the Medical College hospital, to be afterwards disposed off in the same way.[73] This was possibly the reason why, unlike in England, there was no need for a replica of the 1832 Anatomy Act in colonial India. The body was colonized, powerless, devoid of any ‘agency’ and cadavers were plentiful. Harrison remarks, “In Britain, the supply of bodies for dissection was still severely restricted, but there was no such constraints in the colonies, where cadavers were plentiful.”[74]
In eight years, from 1837 to 1844, nearly 3500 bodies were dissected.[75] This was an incredible figure! There seems to have been a never ending supply of unclaimed bodies of hapless poor Indian people. “Every one (sic) knows that this city contains thousands of poor strangers, of all ranks, without wealth, connexion, or friends, who when afflicted with disease, fly from the city, and receiving medicine, and the prescribed regimen elsewhere, recover: but some die on the road, and many perish for want of two pice (sic) worth of medicine. Those who live from hand to mouth cannot obtain proper food or medicine, and for them there is no relief. Those who have no attendance, and no means of obtaining medicine, perish of course by hundreds in the city.”[76]
The military necessity of medical training was explicitly described in the Report (1844-45).
The exigencies created by the war in Affghanistan (sic) and China, led to a temporary increase of the number of all grades of the subordinate Medical Department … During the late war, two apothecaries were sent to China from Calcutta in medical charge of Transports with troops on board, in consequence of the great paucity of medical officers at the presidency at that time. It is in time of war that the good effects of having a well trained set of young men in the subordinate medical department would be most felt…[77]
Under the heading “Remodelling of the system of education”, it was decided that –
The means of instruction, dissecting-rooms, museums, library, laboratory, &c. are such as fairly to entitle it to rank with any of the provincial schools of Great Britain, or the second class schools of medicine, in the Capitals of England, Scotland or Ireland. The chief and insuperable drawbacks to its present recognition, are the divisions of the courses of lectures, and the time occupied by some of them: it being a rule of most European Colleges, that no single Professor shall teach two distinct branches of medical science, except in the cases of Anatomy and Physiology, and Materia Medica with Medical Jurisprudence, and that none of the systematic courses of lectures shall consist of less than 70 lectures or demonstrations upon each subject … It is deemed of great importance that every course of lectures should be of the nature and duration, adopted as the standard of the Royal College of Surgeons … would aid in placing the Medical College of Bengal upon a proper footing, as compared with similar Institutions in Europe.[78]
Three important issues are to be noticed here – (1) the mention of ‘laboratory’, (2) remodelling the system of education to be made at par with “any of the provincial schools of Great Britain, or the second class schools of medicine, in the Capitals of England, Scotland or Ireland”, and (3) following European colleges “no single Professor shall teach two distinct branches of medical science, except in Anatomy and Physiology, and Materia Medica with Medical Jurisprudence”. It was also stated that “the College Council beg to recommend, that the present Professor of Chemistry and Materia Medica, be directed to give annually a course of lectures upon those parts of Medical Jurisprudence, not treated in the toxicological department of the Materia Medica lectures, and that his designation be changed to that of “Professor of Materia Medica and Medical Jurisprudence.”[79]
In accordance with the arrangements above sanctioned, and in compliance with the Regulations of the Royal College of Surgeons, the following was the extent and divisions of the courses of lectures, “to be hereafter given in the College during each Session:
—
Anatomy and Physiology—120 lectures, viz. three lectures a week during the hot, and four during the cold weather, from the 1st of November to the 15th of March inclusive.
Demonstrations and Dissections.—-The latter from the 15th of October to the 15th of March inclusive; the former by three demonstrations a week, during the entire Session, viz. from the 15th of June in one year to the 15th of March of the succeeding year.
Surgery.—The course to commence on the 15th of June, and consist of not less than 70 lectures.
Theory and Practice of Medicine – Same as above
Chemistry and Practical Pharmacy – Ditto
Materia Medica and Therapeutics – Ditto
Midwifery with practical illustrations – Ditto
Botany – Ditto
Medical Jurisprudence.—The toxicological portion to be given with the regular course of Matera Medica; upon the remainder, one lecture a week from the 15th of October to the 15th of March inclusive.
In addition to the above every pupil will be required to compound medicines in the College Dispensary for at least six months, under the charge and direction of the House Surgeon and Apothecary, who has been authorized to grant certificates of proficiency for the same.”[80]
Let us re-examine the question of caste again, even in 1844-45 session.[81] Undoubtedly, caste was an underslying and living aporia within the supposedly secular medical education.
From this session (1844-45) “Title of Students” who have passed all the required subjects after successful completion of their studies, was changed from “letters testimonial” to the title of Graduate in Medicine and Surgery of the Bengal Medical College. It had been granted by Government to all passed students of the Institution, “both to give them a status and consideration among the native community, and as a just reward for the strict and searching examination which each is subjected, prior to receiving this diploma.”[82]
I have mentioned above that how Indian contributions – be it in cash or kind – were erased from government reports – “The College originally formed the Petty Court jail of Calcutta, and all subsequent additions to it have been made at the expense of Government in the Education Department.” Similar things happened again during the establishment of the Fever Hospital – “In reply to Dr. Mouat’s letter, Sir J. P. Grant, the President of the Committee, stated that as Government, under the circumstances of the present financial means of the committee, were unwilling to incur any additional expense, such as might be defrayed by the Calcutta community—the Committee were desirous of ascertaining whether in the event of the Hospital being connected with the College, the officers of that Institution would undertake to afford to the patients the requisite supplies of provisions and medicines, medical and other attendance, necessary to their treatment.”[83]
At this juncture Indian help came to the rescue of the Fever Hospital – “All these conditions were at once complied with by Government and the Council of Education, and while the subject was under the consideration of the Committee, Baboo Muttyloll Seal munificently presented a piece of ground, valued at 12,000 rupees, in the immediate vicinity of the College, for the purpose of aiding to form the site of the proposed Hospital.”[84] Indian contribution was registered in government report too.
To note, the immediate cause of establishing the Fever Hospital was explained in the Report – “The average amount of sickness existing in Calcutta at all times and from every cause, in a fixed and floating population, which has been estimated at 3,00,000 persons, is 18,000, and of these at least one-fifth, or about 3,000 persons die before the end of each year from acute attacks of Fever, or its numerous dangerous and fatal sequelae, without adequate shelter, clothing, food, or medicine of any description.”[85] It was also mentioned that “a small Hospital, containing only 200 beds, would be capable of receiving and discharging 600 patients labouring under the acute forms of Fever every month or 7,200 patients in the year. If the Hospital should contain 300 beds – and a smaller one would be quite inadequate to the demands for assistance – the number relieved in a month would be 900, or in a year 10,800, a small proportion of the sick” Despite this fact one of the worrying facts was – “a large number of persons to be annually rescued from the certainty of death, and placed where each is within a reasonable hope of recovering, and where it is certain that the great majority will recover”[86] And “It would afford relief to the poor Hindoos of every caste, poor Mussulmans, poor Christians, poor Jews, and the many indigent strangers in the city, who resort to it from all quarters to beg, or gain a livelihood by honest industry.”[87]
There were visible changes in the examination system.
The system of examination has likewise been somewhat modified, and more nearly assimilated to that which obtains in most European Universities. Each Professor now examines in his own department, the subject being dictated and determined only by the superintending examiner and assessors, with whom alone rests the decision as to the passing or rejection of the candidate. Besides a written and a practical examination in the dissecting room, every final student is subjected to special trial for twenty minutes at least, in each and every department of study pursued within the walls of the College. The ordeal is much more difficult and extended than that to which candidates for the diploma of the Royal College of Surgeons of England are subjected, and with the exception of Latin, Natural History, and Medical Jurisprudence, embraces every thing (sic) required from a Graduate of the University of Edinburgh.[88]
It signifies that there was a thorough overhauling of the system of medical teaching, examination pattern and the title of the degree awarded to the passed students, with a view to bring the College in close conformity with the best institutions and regulating bodies of Europe. It is substantiated more from a letter jointly signed by the Council of Education and Government – “The approaching departure of Professors Goodeve and Raleigh, has been deemed an eligible opportunity for remodelling the system of instruction pursued at the Medical College, so as to bring within the regulations of the Royal College of Surgeons of England, that institution may be duly registered and recognized, and those of its pupils who may hereafter visit Europe for the purpose of graduating or obtaining the diploma of surgeons, may be enabled to derive the benefit of the time passed here, being allowed to count in other schools and hospitals, as they are at present.”[89]
As a result, “In 1845 the chairs were rearranged to some extent, as noted above, in order to meet the requirements of the examining bodies in London, the University, College of Surgeons, and Society of Apothecaries. In 1846, these bodies recognised the medical education given in Calcutta as qualifying for their examinations.”[90]
First Educational Sojourn
Following all these changes and remodelling, four of the best students of the CMC sailed for their sojourn to England by the ship Bentinck on 8th March, 1845. The background happenings and vicissitudes in the management of monetary questions related to their journey should be mentioned in a detailed way.
One of the most important gratifying occurrences of the past year, has been the munificent offer of Dwarkanath Tagore, to take to England and educate at his own expense, two pupils of the Medical College. This proposal was first communicated to Dr. Mouat, who announced it to the assembled school, and pointed out the great advantages that would resu.lt to any one bold enough to break through the trammels of caste, and profit by the opportunity offered of visiting Europe. Upon this, and almost immediately after the address referred to, three students volunteered unconditionally to go, viz. Bholanath Bose, Surjee Coomar Chuckerhutty, and Dwarakanatlh Bose—a fact so highly creditable to their spirit and anxiety to profit by the liberality of their distinguished countryman, as to deserve special record. Subsequently to this, Professor Groodeve offered to proceed to Europe in charge of the pupils who might be selected, to superintend their education, and to pay from his own funds the expense of an additional student, on condition of certain benefits being extended to him by Government, for making so great a sacrifice as the preceding, if agreed to, would entail upon him … The advantages of the scheme will be great, both as exhibiting the nature and extent of the medical education which can be given to the pupils in Calcutta, and also of elevating them in the estimation of the Native community, should any of them return with European Diplomas, which they are fully qualified and able to obtain …. Dr. Goodeve succeeded in raising an additional sum of 7,500 rupees for a fourth student, 4,000 of which were munificently presented by his Highness the Nuwab Nazim of Bengal.[91]
The fourth student was Gopal Chandra Seal. As we see from this description, truly speaking, government had borne only the cost of single student. Rest three were financed by Dwarakanath, Nawab Nazim of Bengal and Dr. Goodeve. Such was the extreme parsimony practised by the East India Company. It was their inherent practice of ‘economy of education’. In most cases government was only the granting authority. But a great part of any institution was actually borne by local people and public subscription.
Regarding the four student making their journey of England, the Report said – “The four pupils who accompanied the Professor and started in the Steamer Bentinck on the 8th March, were Bholanath Bose, a pupil of Lord Auckland’s School at Barrackpore, who was supported at the Medical College by His Lordship for five years, and was considered by the late Mr. Grifiith, the most promising botanical pupil in the school—Gopaul Chunder Seal—Dwarkanath Bose, a Native christian, educated in the General Assembly’s Institution, and employed for some tune as assistant in the museum—together with Surjee Coomar Chukerhutty, a Brahmin, native of Commillah, a junior pupil and a lad of much spirit and promise.”[92]
According to Gorman, this educational sojourn had three-fold effects – (1) it showed convincingly that Indians could master science and medicine on a level with Europeans; (2) having attained their degrees from the UCL (University College London) and the Royal College of Surgeons, they served as disseminators of modern science and became role models for future Indian students; (3) their example set the stage for a veritable flood of Indian students to England for study in all fields which continues to this day. They studied under the famous Thomas Graham – the innovator of Graham’s Law in chemistry.[93] More elaborately speaking, Gorman describes the entire stage in the following manner.
The choice of this institution bears comment. It s medical school was widely regarded as the most progressive and innovative in Europe, and consequently attracted the highest calibre of students in England and from abroad. The faculty of the Calcutta Medical College were well aware of this high standing, and constantly sought to imitate its best features. It never occurred to them to choose one of the lesser schools of London or the province, so confident were they of their students that they selected deliberately the toughest competition. Most English men would not have expected these Indians from a disease-ridden, superstitious frontier outpost to have the slightest chance of success. Even one acquainted with the faculty, curriculum, and standards of the Calcutta Medical College would have been satisfied to have these students pass with average records at University College. They were far from home without social support from family or friends and they were studying in a foreign language. They could easily have been overwhelmed by the accomplishments of their classmates and the prestige of the faculty, but results proved that any such negative expectations were groundless. They not only passed, but did so with distinction, winning gold and silver medals and certificates of honor in various subjects from anatomy, botany, and chemistry to zoology. Their academic exploits were noted in the press.
Various official reports of University College and the East India Company gave them the highest possible praise. Space does not permit a detailed description of the demanding standards they had to meet for an understanding of the subjects presented to them, but as an example of the quality of the faculty it may be noted that for chemistry Thomas Graham (1805-1869) was their teacher. He is remembered today as the discoverer of Graham’s Law, and in his time was the “acknowledged dean of English chemists.”[94] McCully has informed us that after the CMC students’ first sojourn to England/Europe for higher education more than 700 students made their journey to England “to complete their education” between the years 1865 and 1885.[95]
Some interesting facts about Bholanath Bose can be enumerated. Auckland had founded Barrackpore School where Bohalanth was student. Auckland himself transferred Bholanath when he was 16 years old, the brightest student of the school, to the CMC in 1840 with a scholarship of Rs. 10 per month.[96] Finishing his education at the UCL, on the eve of departure for Calcutta, Bholanath received a touching letter from Auckland on 13 January 1848 –
“My dear Bholanath,
I will not allow you to leave England without writing a few lines to you to say that I wish you well. I would add too that you have given very great satisfaction to me and to your other friends, by the earnestness with which you have pursued your studies, and by distinctions which have attended your success in them.
I should like you to take away with you some token of remembrance from me, and I will beg you purchase one that may be agreeable to you with the enclosed draft.
Yours most truly, &c.,
Auckland”
“With the amount of this draft Dr. Bose bought a gold watch, which according to the terms of the Doctor’s will, is to be preserved as an heirloom in the family.”[97]
Moreover, College Council seems to be more concerned with the positive social effects this voyage could generate.[98] It was joyously noted in the report of the 11th Year – Session 1945-46 – of the CMC that “[a]mong the most gratifying, striking and important events of the session which has recently closed, has been the recognition of the Bengal Medical College by the Royal College of Surgeons of England, the University of London, and the Worshipful Society of Apothecaries. This is the first instance of any of the educational institutions of British India being granted the privilege of preparing pupils for the academic and professional rewards of corporate and chartered bodies in England.”[99] It was no doubt a great achievement of a medical college of the colonies. This recognition meant that less time would be required to pass the examinations from those reputed international institutions. Early training in the CMC could be regarded at par with those institutions.
Final Remarks
Following the recognition of the CMC by the most prestigious and influential institution and bodies of England, it was gleefully reported –
The pupils of the medical college will be permitted hereafter to present themselves for examination before any of the bodies above-mentioned, for the purpose of obtaining the degree, diploma, or license, which they respectively afford, by passing through the particular course of study indicated and required by each. The college possesses the means of affording all the purely professional instruction necessary, without residence or study in any other country or institution; the value of the boon accorded can therefore be scarcely overestimated.[100]
It was a matter of great pride that the CMC was the first ever institution beyond Euro-American borders to be recognized by the institution and bodies mentioned above. The professional training at the CMC was so methodical, meticulous and rigorous that the students of the CMC, after a short period of probation, could sit for examinations like M.D., F.R.C.S. or M.R.C.P. and more in the institutions of England and Scotland. This was a feat of great honour, and indelibly changed the course of medical education in India forever.
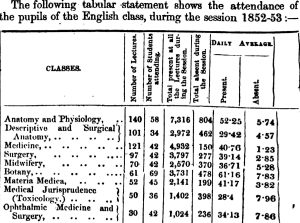
The immediate impact of advanced European education after the recognition from England was convincingly felt later in the annual report of the session 1852-53. The report stated – “Mr. Marcardieu was appointed to the temporary charge of the laboratory, and a communication was addressed to the Government, soliciting the appointment of a Chemist from Europe, to teach the science in all its departments, to its present standard of progress in Europe.”[101] Moreover, from the same report we come to know that Dr. Chuckerbutty was appointed as the assistant physician in the Medical College Hospital.[102] Following table shows how the entire syllabus, subjects and classes were made to suit its recognition accordingly.
Allan Webb, in his ‘Introductory Lecture’ in June, 1950, informed the students – “Dwarakanath Bose was the first of our gallant band of medical pioneers, to return to us with the diploma of the Royal College of Surgeons. He is now your teachers (sic) of Anatomy. Surjoo Coomar Chuckerbutty, just returned with the diploma of the London University, is Assistant Physician in our College Hospital. Drs. Seal and Bose both held appointments in the City.”[103] Such was the outcome of the great sojourn to England/Europe, which indelibly changed the course of medical education in India forever.
____________
[1] W. H. Sykes, “Statistics of the Government Charitable Dispensaries of India, Chiefly in the Bengal and North-Western Provinces”, Journal of the Statistical Society of London, Vol. 10, No. 1 (Mar., 1847): 1-37 (11). [Italics in original]
[2] Ibid, 12. [Italics added]
[3] C. A. Bayly, Empire and Information: Intelligence gathering and social communication in India, 1780-1870 (New Delhi: Cambridge University Press, 2007), 265.
[4] Dipesh Chakrabarty, “The Difference-Deferral of a Colonial Modernity: Public Debates on Domesticity in British Bengal”, Subaltern Studies, Vol. VIII (New Delhi: Oxford University Press, 1996): 50-88. Quoted on pp. 56-57.
[5] Sykes, idem, 22.
[6] Ibid.
[7] Ibid, 22.
[8] Thomas Farquhar, “Progress of Dispensaries in India”, Lancet, Vol. I (May 14, 1870): 690.
[9] Ibid.
[10] Ibid, 691.
[11] Jacques Derrida, Aporias (Stanford: Stanford University Press, 1993).
[12] GCPI 184041 & 1841-42, 82.
[13] Ibid, 83.
[14] Ibid, 85.
[15] Ibid, 91.
[16] Ibid, 92.
[17] Ibid, 94.
[18] Ibid.
[19] Michel Foucault, The History of Sexuality: An Introduction, Volume 1 (Vintage Books: New York, 1990), 139.
[20] GCPI 1840-41 & 1841-42, 95. [Italics added]
[21] Ibid, 97.
[22] Ibid, 98.
[23] Ibid, 100-101.
[24] Ibid, 104.
[25] Ibid, 107-110.
[26] GCPI 1840-41 & 1841-42, Appendix No. X, lxxi. [Italics added]
[27] Ibid, lxxxv.
[28] Ibid, lxxiv.
[29] Ibid, lxxiii.
[30] Ibid, lxxxvii. From H. H. Goodeve’s report written on Febrary7, 1842. He was the Professor of Midwifery Department.
[31] Ibid.
[32] Ibid.
[33] Ibid.
[34] Ibid, lxxxviii.
[35] Ibid.
[36] H. H. Goodeve, Hints for the general management of children in India in the absence of professional advice (Calcutta: W. Thacker and Co., 1844).
[37] Goodeve, Hints for the general management of children in India in the absence of professional advice , 4th edition (W. Thacker and Co.: Calcutta, 1856).
[38] GCPI 184041 & 1841-42, Appendix No. X, lxxxiv.
[39] Ibid, lxxiv.
[40] Ibid, lxxx-lxxxi. [Emphasis in original]
[41] Ibid, Appendix No. XII, xciv. [Italics added]
[42] General Report on Public In the Bengal Presidency, for 1842-43 (hereafter GRPI), 90. [Italics added]
[43] GRPI, 1842-43, 78-79.
[44] Ibid, 79.
[45] Ibid, 80.
[46] Ibid, 80-82.
[47] Ibid, 84.
[48] Ibid.
[49] The Medical College of Bengal (Calcutta: W. Rushton & Co., 1839), 7.
[50] Ibid, 8.
[51] GRPI, 1842-43, 86. [Italics in original]
[52] Ibid, 87.
[53] Emma Roberts, “The Medical Service and Its Prospects”, Parbury’s Oriental Herald, July-December 1838, 2 (IX): 245-252. Quotation on 251-252.
[54] Ibid, 245.
[55] Ibid, 250.
[56] Centenary, 14.
[57] “Flourishing State of Medical College of Bengal,” The London Medical Gazette or Journal of Practical Medicine, New Series, Vol. V (1847): 126-127.
[58] Jayanta Bhattacharya, “Arrival of Western Medicine: Ayurvedic Knowledge and Colonial Confrontation”, Indian Journal of History of Science, 2011 46(1): 63-108. Quotation on p. 92.
[59] GCPI 1840-41 & 1841-42, 94.
[60] Ibid, 95.
[61] Ibid.
[62] Ibid, 96.
[63] Thomas Neville Bonner, Becoming a Physician: Medical education in Britain, France, Germany, and the United States, 1750–1945 (New York, Oxford: Oxford University Press, 1995), 144.
[64] GCPI 184041 & 1841-42, 96.
[65] Ibid, 97.
[66] Ibid, 114.
[67] GRPI 1844-45, 99.
[68] Ibid, 106.
[69] GRPI 1845-46, 107.
[70] Ibid, 108.
[71] Ruth Richardson, Death, Dissection and Destitute, (London: University of Chicago Press, 200), 293.
[72] GRPI, from Oct. 1850 to 30th Sept. 1851, 81.
[73] C. E. Buckland, Bengal under the Lieutenant Governors; being a Narrative of the Principal Events and Public Measures during Their Periods of Office, from 1854 to 1898, in 2 volumes, I (Calcutta: S. K. Lahiri & Co., 1901), 296.
[74] Mark Harrison, Medicine in an Age of Commerce: Britain and its Tropical Colonies, 1600-1830 (Oxford, New York: Oxford University Press, 2011), 4.
[75] Allan Webb, Pathologia Indica, or the Anatomy of Indian Diseases, 2nd edition, in 2 parts (London: Wm. H. Allen & Co., 1848), 237.
[76] James Pegg, India Cries to British Humanity: Relative to Infanticide, British Connection with Idolatry, Ghaut Murders, Suttee, Slavery, and Colonization in India, to which are Added Hints for the Melioration of the State of Society in British India (London: Simpkin and Marshall, 1832), 293.
[77] GRPI 1844-45, 122-124.
[78] GRPI 1844-45, 101-102. [Italics added]
[79] Ibid, 101.
[80] Ibid, 102.
[81] Ibid, 106.
[82] Ibid, 123.
[83] Ibid, 133.
[84] Ibid.
[85] Ibid, 134.
[86] Ibid, 135.
[87] Ibid, 135.
[88] Ibid, 123-124.
[89] Ibid, 101.
[90] D. G. Crawford, A History of the Indian Medical Service, 1600-1913, Vol. 2 (London: W. Thacker & Co., 1914), 441.
[91] GRPI 1844-45, 118-119.
[92] Ibid, 119.
[93] Mel Gorman, “Introduction of Western Science into Colonial India: Role of the Calcutta Medical College”, Proceedings of the American Philosophical Society, Sep., 1988, 132( 3). 276- 298. Quoted on p. 290.
[94] Ibid, 290.
[95] Bruce Tiebout McCully, English Education and the Origins of Indian Nationalism (New York: Columbia University Press, 1940), 215.
[96] Ramgopal Ghosh, ed., Reminiscences and Anecdotes of Great Men of India, Both Official and Non-official for the Last One hundred Years (Calcutta: Herald Printing Works. 1894), 72.
[97] Ibid, 72-74.
[98] Regarding the four most illustrious students of the CMC, they showed their brilliance and merit in University College, London, in the same way as in India. Bholanath Bose stood 3rd for the Botanical examination among more than 70 students. He missed the 2nd position only by two marks. Gopal Chunder Seal was selected by no other Professor Quain to dissect the subjects for his lecture – a post of considerable honour in the anatomical class. Suraj Coomar Chuckerbutty has by his zeal and attention so completely won the regard and approbation of Dr. Grant, the distinguished Professor of comparative anatomy. Dr. Grant had also presented him with copies of all his own works, and many of the most important treatises on this subject published in this country and in France, moreover he took Chuckerbutty with him to Paris. (Dr. Goodeve’s Report on the progress of the students in London, GRPI 1845-1846, 111).
[99] GRPI 1845-1846, 110.
[100] Ibid, 110.
[101] GRPI, From 30th Sept. 1852, to 27th Jan. 1855, 63.
[102] Ibid, 61.
[103] Allan Webb, The Historical Relations of Ancient Hindu with Greek Medicine … Being a General Introductory Lecture Delivered June 1950 (Calcutta: J. C. Sheriff, 1850), 5-6. [Italics added]










My regards and appreciation to you, Dr Jayanta Bhattacharya, for wonderfully correlating different aspects of the history of of the great CMC from contemporary records and references. We got the prize institution at the initiative of some dedicated British social workers and medical scientists ably supported by contemporary enlightened local aristocrats though their contributions were carefully understated by the the British administration.
But ultimately we got the new system of treatment which had more curative and life-saving effects and which never maintained and caste boundary both for the doctors and the patients.
Thank you, Dr Jayanta, for presenting us such rich articles. CMC may have lost some glory at present, but, I am sure, it would come back soon.
Thank you!
Brilliant piece of work on CMC, it’s training and its contribution to the development of western medicine through dispensary system. The reorganisation and periodic improvements have delivered the required goals. Also the changed attitude in the public especially the caste system based attributes have been written. Scholarly work 👏🏽👏🏽