

Early days of Western medicine in India was not much conducive to the British settlers and Indians as well. Though, it is historically accepted that doctors played a prominent, rather most conclusive, role in the foundation of the British empire. British Medical Journal termed them as “MEDICAL EMPIRE BUILDERS”. Two men are especially discussed in this regard. First one is Gabriel Boughton, and the second one is William Hamilton.
Crawford has discussed at length about these two personalities in his magnum opus. According to Crawford, under the title “The Legend of Gabriel Boughton”, “One of the most widely known stories of the early history of the English in India is the legend of Gabriel Boughton, Surgeon of the Hopewell; how he was sent for to attend the daughter of the Emperor Shah Jahan, who had been badly burned; how he was successful in effecting a cure ; and how, when desired to name his own reward, he asked for and obtained liberty for his masters, the Company, to trade in Bengal, after which the first settlement of the East India Company in Bengal was founded.”
Interestingly, Italian traveller and self-taught physician Nicolao Manuci was present during the event of burn of the Emperor Shah Jahan’s daughter Jahanara Begam about the year 1636. He has also mentioned about the incident. But he is silent about her treatment – “This Princess treated herself to many entertainments, such as music, dancing, and other pastimes. It happened one night while engaged in such-like dances that the thin raiment, steeped Princess’s favourite dancing woman caught fire, and she bore to her, the Princess came to her aid, and thus was burnt herself on the chest.”
It is learnt from another account that “About the year 1636, there was one Gabriel Boughton a chyrurgion at Madras … In the year of the Hezira 1046 (A.D. 1636), a daughter of the Emperor Shah Jehan having been dreadfully burnt … Mr Gabriel Boughton, Surgeon of the ship Hopewell who immediately proceeded to the Emperor’s camp, then in the Deccan”. Moreover, as reported, after curing Jahanara Boughton “sought not for any private emolument, but solicited that his nation might have liberty to trade, free of all duties, to Bengal, and to establish factories in that country.”
Crawford notes, “That Bridgman succeeded in obtaining a farman from Shah Shuja, presumably by the aid of Boughton, is shown in a letter from Madras dated 14th Jan., 1651/52 (0. C. 2246), quoted by Foster … The loss of this farman is narrated as follows in a letter from Madras to the Company, dated l0th and 22nd Nov., 1656 (0. C. 2579), also quoted by Foster”. But, finally comparing all historical sources that are often conflicting, Crawford come to the conclusion – “Little more is known of Boughton with any certainty. Neither the date nor place of his death seems to have been recorded. He was alive in Jan., 1651/52, and died in 1653 … Whatever may have been Boughton’s services in obtaining a farman for the Company, long before his time the Company’s servants at Surat had tried to obtain liberty to trade, free of custom with Bengal.” Again, “The date and place of Gabriel Bonghton’s death are unknown. No stone marks his resting place, no memorial to him is in existence. His name is not even mentioned in the Dictionary of National Biography. But History records his services to the Company and to his country.”
Regarding William Hamilton, Crawford has noted, ““Of all the medical officers who have served in India during the past three centuries, William Hamilton is probably the most famous, and is certainly the one who has been the greatest benefactor of his country.” In contrast to Boughton, Crawford comments, “The story of Gabriel Boughton may be in part apocryphal, but there is no doubt of the reality of the services of William Hamilton to his country, and to his masters, the E.I. Co. Yet his name does not appear in the Dictionary of National Biography”.
Later on, we come to know about Hamilton thus – “when an important embassy went from Calcutta to the Emperor, Farekh Siyar, in 1714, it was the skilful treatment of the Emperor by the Company’s Surgeon, William Hamilton, a cadet of the family of Hamilton of Dalziel, that eventually obtained important concessions upon which the subsequent prosperity of the Company largely depended.” Hamilton was also one of the doctors who performed first recorded post mortem in Calcutta – “In the same year, 1713, Hamilton and Harvey performed a post-mortem, the first in Calcutta of which any record has been preserved, as noted in Cons, of 6th Aug., 1713”. In a more detailed official account – “Doctor Hamilton and Doctor Harvey deliver’d us the following certificate relating to the death of Wm Hall according to the order of Consultation of 30th Ult°.
We do declare according to the best of our Skill upon the opening of the Body of Wm Hall who had recd a wound by a Rapier m the lower part of his Belly on the right side obliquely passing under the Gutts wounding the Coats, the Narves of the Kidneys, Emulgent Arteries & great Lacteal Veins from which wounds he reced his death.”
When Hamilton reached Delhi the Emperor had been suffering from a lesion in his groin. “The first distemper the doctor took him in hand for, was swellings in his groin, which, thanks be to God, he is in a fair way of curing; but within these few days last past he has been taken with a violent pain which Is likely to come to a fistula”. As a result of Hamilton’s surgical and medical skill the Emperor was relieved of his excruciating pain and much pleased. From report of December7, 1715, it is known that Hamilton had received huge amount of royal gifts – “As a reward for Mr. Hamilton’s care and success, the King was pleased on the 30th to give him in public, viz., a vest, a culgee (a turban ornament) set with precious stones, two diamond rings, an elephant, a horse, and 6,000 rupees; besides ordering at the same time all his small instruments to be made in gold, with gold buttons for his coat and waistcoat, and brushes set with jewels.”
According to Crawford, “Hamilton was richly rewarded, receiving an elephant, a horse, five thousand rupees in money, two diamond rings, a jewelled aigrette (refers to the tufted crest or head-plumes of the egret, used for adorning a headdress), a set of gold buttons, and models of all his instruments in gold.” Along with this, the most coveted prize he received from the Emperor was the permission free trade in Bengal by the East India Company (hereafter EIC).
Hamilton died on 4 December, 1717, in Calcutta. His demise was also deeply felt by the Emperor himself. His tombstone at St. John’s Church, Calcutta bore an inscription in Persian too. Original inscription on tombstone read thus –
Under This Stone Lyes Interred
The Body of
“William Hamilton, Surgeon,
Who departed this life the 4th December, 1717.
His memory ought to be dear to his
Nation for the credit he gain’d the English
in curing Ferrukseer, the present
King of Indostan, of a
Malignant Distemper, by which he
made his own Name famous at the
Court of that Great Monarch;
and without doubt will perpetuate
his memory, as well in Great Britain
as all other Nations of Europe.”
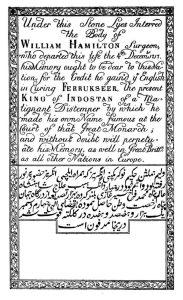
(William Hamilton’s gravestone)
At the time of William Hamilton another traveller Alexander Hamilton (? 1688-1733) came to India. In his sarcastic account he lets us know – “The Company has a pretty good Hospital at Calcutta, where many go in to undergo the Penance of Physick, but few come out to give Account of its Operation.”
Western medicine, specifically in the area of medical treatment, cut a sorry figure, rather was in a deplorable condition. In the realm of surgery it excelled no doubt, as we have already seen in case of William Hamilton’s surgical skill.
It is known from a report of 1767, under the title “Medicines, Price and Class” (entry number 960) – “it is considered that near five thousand Europeans partake yearly of the Hon’ble Company’s medicine, besides sepoys and other black people in their service”. What type of medicines was actually needed? It cannot be ascertained for certain. But from another account it can be understood to an extent.
In September, 1767, Jagat Set, one of those who wholeheartedly colluded with the British in the overthrow of the Nawab of Bengal in 1757, complains in a letter of his shoulder being “disjointed” having slipped on plain ground, and that “I have not got the use of my arm” and asked for medicine to unknown British authority. In response to this “Medicine for Jagat Set” (entry number 494) was sent. The British medicines sent for his cure were some kind of “oil and extract of horn and other medicines wrapt in paper for the cure of Juggut Seat’s (sic) arm dislocated by his foot slipping”.
Against this perspective, Bayly’s comment may be put and properly appreciated – “When the British denounced Indian backwardness in theory, they meant their continued adherence to Aristotelian humoral notions which had only recently been abandoned in Europe. The insecurity of European knowledge was a potent element in their rages.”
For an extended perspective, from a different perspective, the idea of being admitted into a hospital was not nor is historically palatable to the patient. As far back in 1924, Lushington, a British Whig politician and secretary to the Bengal Presidency, commented – “The idea of entering a Hospital for relief, though it is usually administered with skill and humanity, is repugnant to the feelings of the meanest individuals, and excites a sensation of forlornness even in minds strengthened by education.” Similar view is echoed in the most celebrated textbook of internal medicine – “The hospital is an intimidating environment for most individuals. Hospitalized patients find themselves surrounded by air jets, button, and glaring lights; invaded by tubes and wires … It is little wonder that patients may lose their sense of reality.” Even in mid-19th century American experience, regarding hospital, “People feared that physicians would experiment on patients and that inexperienced students would cause harm.”
Glimpses of Early History of Medicine in Colonial Bengal
The first hospital in Calcutta was opened towards the end of 1707 or early in 1708. Its construction was ordered in Fort William Public Cons, of 16th Oct., 1707. “The Bengal Cons., of 13th Feb., 1709/10, contain the following note on this hospital :—“There being a great many Europe Soldiers in the Garrison who if they lodge about the town as Vsually (sic) will create sickness and other inconveniences to themselves and others therefore tis “AGREED the Hospitall be walled round and that Barricks be made in it for the Soldiers to lodge in and that some of the Officers doe likewise lodge there and see a good Decorum kept amongst them.” The hospital was again in great want of repairs in 1754. The Cons, of 25th July, 1754. This first Calcutta hospital, to which all the above entries refer, was destroyed at the capture of Calcutta in June. 1756.
“A new hospital, however, had been provided before the old one was sold. In Cons, of 29th Sept., 1766, it was resolved to remove the old hospital and burial ground, and to build a new hospital. The graveyard thus closed was the old one, where St. John’s church now stands. It contained the bodies of all Europeans who had died in Calcutta since 1698, (probably about 12,000” .
Crawford brings an interesting fact to our notice – “The Hospital Regulations of 1713 show that cots were then provided for the sick. How these cots differed from the beds now wanted is not apparent; possibly the cot was a swung hammock, or a fixed bunk, like those on board ship. It can hardly be supposed that the sick slept on the damp floor. At this period, 1752, the hospital had two stories; the Surgeons’ Mates lived in an unboarded room on the ground floor.”
The hospital at Ghireti was for sipahis. A similar hospital, more than twenty years earlier, is mentioned by Captain Fenwick as suggested at Dean’s Town, i.e. Dane’s town, a place where the Danes had a thatched house on the west bank of the Hugli, south of its junction with the Rupnarayan, and opposite Hugli Point, about where the modern town of Giankhali now stands.
Most likely, this hospital at Ghireti was located in the present town of Chandanangar, Hugli district. Serampore is located about 20 km north of Kolkata and like Bandel, Chinsurah and Chandannagar, is located on the right bank of the Hooghly River. Serampore was a Danish colony from 1752 to 1845, and was known as Fredrick Nagar after the Danish King Frederick VI.
The Cons, of 16th Nov., 1767 record that Mr. Kiernander’s garden house is to be surveyed by the Chief Engineer, the Surgeons and the Civil Architect, who will report if it will do for a hospital. A le1tter from Mr. Kiernander about the conversion of his house into a hospital is entered in Cons, of 4th April, 1768. On 25th April is recorded the payment of Rs.98,900 to Mr. Kiernander for this house. A Letter to Court, dated 13th Sept., 1768, reported in para. 65: “Hospital, Revd Mr Kiernander’s House purchased for one at Rs. 98,000 and have been contracted with him for building the additional buildings thereto.”
This may be said to have been the third hospital erected in Calcutta. The first was that of 1707-08, and the second the temporary makeshift in the Fort, from 1757 to 1769. All three were primarily intended for the Company’s soldiers and sailors, but admitted all Europeans, of all classes and of all callings. The last one was between 1902 and 1908 replaced by the magnificent buildings of the new Presidency European General Hospital.
The admissions to hospital from 1st Sept., 1805 to 31st Aug., 1806, were as follows: Wounds 77, Fractures 34, Venereal 4, Contusians (sic) 18, Scalded and burnt 4, Dropsy 7, Abscess 8, Fever 15, Palsy 2, Dysentery 2, Fistula in ano 1, Stranguary 5, Locked jaw 2, Spleen 3, Rheumatism 2, Cancers 2, Ulsers and sores 21, Excessive vomiting 1, Tumours 1, Dislocations 1, Concussion of brain 3, Mortifications 3, Cholic 2, Catarrh 1, Scurvy 1.
Total 220. [Spellings are retained as in original]
“The C.G. of 18th Oct., 1792, notifies that it is intended to institute a hospital for natives.”
For Indians, Calcutta Native Hospital was established 1792. More importantly, this hospital “appears to have been the first institution to provide scientific treatment for diseases of the eye”
The C.G. of 18th Oct., 1792, notifies that it is intended to institute a hospital for natives. The same paper, on 1st Nov., 1792, states that a meeting had been held, at which it was determined (1) to institute a hospital for natives; (2) to vest the management in an equal number of European and Native Governors, residents of Calcutta; (3) to appoint a Committee to raise subscriptions and prepare a plan.
Government granted a subsidy of Rs.600 a month, on 6th July, 1793. Twelve Governors were appointed. The first hospital was opened in a house in the Chitpur Road, subsequently a house in Dharamtola was bought, and opened as a hospital on 1st Sept., 1794.
Mark Harrison draws our attention to the fact that these hospitals “One striking feature of admissions to these hospital in their early years is that there were three times as many in-patients as out-patients, which suggest that the hospitals were seen more as shelters for the indigent than as curative institutions”
From The Diaries of Streynsham Master 1675—1680 we come to know of an Indian doctor named Nilkanth. From an entry on October 22, 1676, it is known that “The Indian Doctor, who was sent for to cure Major Puckle (he haveing cured Mr. March of the like Distemper) came this day from Hugly” . They were termed as “Black Doctors”. Broome gives us an account of 8,338 black doctors – 2 black doctors for a battalion of 1,000 armies. The earliest reference to ‘black doctors’ is possibly found in a return of the Company’s Bengal Army on 21 June 1762. There were 19 “black doctors” among 8338 English soldiers, or about two per battalion of a thousand men. When the Company raised a standing army, native medical attendants were appointed to each crops and regiment.
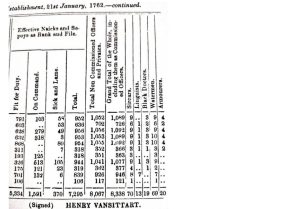
(From Arthur Broome, History, Appendix P, XXXI)
A Government Order (GO) of 15 June 1812 approved of a plan submitted by the Medical Board for training boys from the Upper and Lower Orphan Schools and from the Free School, as compounders and dressers, and ultimately as apothecaries and sub-assistant surgeon in Bengal. It was stated that twenty-four boys of fourteen or sixteen years of age were to be selected. They were to be posted as follows—ten at the General hospital at the Presidency, ten at the Garrison Hospital, Chunar and four at the General Dispensary. They were placed under the immediate charge of the Superintending Surgeon. “The Boys thus selected, are to be posted as follows, viz. : — At the General Hospital at the Presidency 10, Garrison Hospital, Chunar 10, General Dispensary, 4.”
“When these pupils are considered by the Superintending Surgeon, and the Surgeons under whom they will be more immediately educated, duly qualified for exercising the duties of Compounders and Dressers, they shall then be stationed at the recommendation of the Medical Board with such native corps as may more peculiarly require their aid; and afterwards with the different European Corps of the Honourable Company’s Service, with Field Hospitals, and with the Depots of Medicines.”
Such medical training was of a purely military nature, to serve only military purposes. Moreover, it was not an institutional training, but rather an individual tutoring under the superintending surgeon with the aim to produce compounders and dressers. It had no syllabus, no proper examination system or certification. The twin need of utter military necessity and economy of education in the production of Native Doctors will be much more evident from observations of Lushington, as regards the formation of the Native Medical Institution (NMI):
The anxiety of the Medical Board, relative to the paucity and inefficiency of that useful body, the Native Doctors, induced them in 1822 to represent the matter to Government, in order that a remedy might be applied to an evil which was rapidly increasing, and threatened the most injurious consequences to the service.
Previously to the abolition of the General Hospitals in the interior of the Country, and the augmentation of the army, persons of this description, properly qualified, were procurable in adequate numbers. But, the sources whence they had acquired their knowledge having been removed, they were no longer to be procured at fixed stations, in cases of emergency, and the Medical staff were obliged to take such individuals as offered, wherever they could be found, notwithstanding their slender qualifications. Thus, by a peculiar fatality, as the demand for Native Doctors increased, so the means of meeting it were diminished. Owing to our recent expansion of territory, and the consequent wide distribution of the army for it’s protection, a great number of the Native Battalions had been broken down into two and sometimes more sub-division.
Lushington further notes that not only military stations, but also the civil stations were not exempt from “the same evil”: “even to a greater degree at the Civil Stations, some of which had from the scarcity of assistant Surgeons been left for long periods to the care of the Natives.” Especially, under such circumstances, “it was not surprising that great mortality evinced the unskilfulness of the Native practitioners.” Being left at the hands of the Native Doctors, though quite unfortunately, seems to denote two aspects – (1) the dwindling of superiority of the White race, as well as (2) superior position of European medicine not being properly applied.
It may be mentioned here that the EIC had engaged them in a series of wars to consolidate their political, economic and administrative power. “On several such occasions, in the Maisur and Maratha wars of 1780-81, the third Maratha war of 1817-18, and the first Burmese war of 1824-25, the Indian Government made numerous local appointments of Assistant Surgeons.” What they needed most was recruitment of Indian boys for military purpose, with basic knowledge of dressing the wounds and administering medicines. For this purpose, some knowledge of anatomy, body organs and surgical skill were direly needed. To understand the dynamics in a better we need to know European surgical excellence done in institution.
Institutional Surgical Excellence and Penetration of European Medicine
On January 1, 1838, a paper by Richard O’Shaughnessy (the then Demonstrator of Anatomy of the Calcutta Medical College) was published in the Quarterly Journal of the Calcutta Medical and Physical Society, under the title “Case of Enormous Tumour of the Upper Jaw” . A slightly revised paper was also published in the esteemed journal Lancet in the same year.
The most intriguing question was – how in the pre-anaesthetic era was removed such an enormous tumour of the jaw? Removal of the tumour demanded a few basic things – (1) efficiency of the surgeon, (2) knowledge about specific and exact anatomical location of the tumour, and (3) swiftness of surgery.
O’Shaughnessy described the tumour as “[t]he tumor weighed four pounds … nearly globular in form, having at its inferior surface a deep groove into which the lower jaw sunk … In making a section right through its axis it was found to be of a dense fibro-cartilaginous structure, surrounded for three-fourths of its entire extent by a pellicle of bone about the thickness of fine parchment”
This description draws our attention to the fact that unlike traditional Ayurvedic or other indigenous medicines, the question “to dissect, or not to dissect” has become redundant in this perspective. It has come a long way from dissection-debate to organ-localization of disease. As a result of which O’Shaughnessy could describe so accurately about the localization and structure of the tumour. Owsei Temkin has succinctly focused on the role of surgery in the rise of modern medical thought – “Surgery, for many centuries, had relied on an objective anatomical diagnosis. In turning to a localized pathology, medicine adopted a point of view prevalent among surgeons … the reorientation of medicine was due to an increasing approximation between medicine and surgery during the 18th century, with pathological anatomy and experimental physiology as a common ground cultivated by both disciplines.”
There is a fascinating history behind the surgery by O’Shaughnessy. And that is the history of the genesis of “hospital medicine” in India and the foundation of the Calcutta Medical College (also variously named as only Medical College, Bengal Medical College or Medical College, Bengal) in Calcutta. It is a well-known fact that by a government order (G.O. No. 28 of 28th January, 1835) the Calcutta Medical College (hereafter CMC) was founded. Along with the foundation of the CMC on 1st February, 1835, it was ordered that “the Native Medical Institution (hereafter NMI) and the medical classes at the Madrasa and at the Sanskrit College being abolished”. The G.O. had thirty five clauses with concrete details about the mode of teaching, staff, stipend and prospective students and more. Clause 15 of the Order read thus – “That all foundation pupils be required to learn the principles and practice of the medical science in strict accordance with the mode adopted in Europe.”
Coming to O’Shaughnessy’s operation of the tumour, it can be briefly stated that Woodey (?Uday) Morrol, aet. 21, a Hindu of the farmer caste, tall, thin and slightly emaciated, native of a village called Pangey, in the district of Kasba, which is a day’s march from Jessore, and about three days’ journey from Calcutta, presented himself at the Gurranhatta Dispensary on the 6th of November.
In O’Shaughnssy’s description – “For the few days he remained in the Dispensary before the operation … So pressing were his entreaties to have it removed that I refrained from having a cast of it taken as that would have caused the delay of an additional day, though I was very anxious indeed to procure one for the museum of the Medical College.” It is interesting to note here that R O’Shaughnessy sought to preserve the excised tumour in the newly opened museum of Medical College. So the patient was transferred to the Medical College. Moreover, he was “taken to the theatre of the Medical College, where, for the advantage of the pupils, and also as having there better light and room than in any apartment in my Dispensary, l thought it best to operate.” Transfer to the Medical College served two more purposes – (1) it would be advantageous for the students of the College to see the whole operative procedure to learn surgery in a better way, and (2) the College had better surgical facilities than a dispensary.
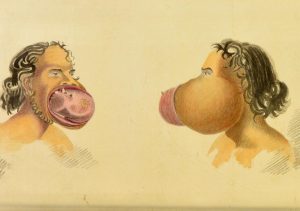
(Jaw tumour of Woodey (?Uday) Morrol – drawing by R O’Shaughnessy, November 1837. Courtesy: Wellcome Collection))
We should again remember that this diccicult and complicated surgery was performed in pre-anaesthetic era, when severe pain and concomitant bleeding was almost a regular phenomenon. However, the patient was seated in a stout arm chair and his head was “supported by Dr. Corbyn, who kindly offered to undertake that charge, while a second assistant, Dr. Goodeve, stood at his left side prepared to make pressure on the carotid artery, if at any time during the operation the bleeding called for such interference” .
We do not need to enter into the operative details of this case. For our relevance, it may be stated that – (1) the patient was sedated with “80 drops of laudanum (an alcoholic solution containing morphine) before the operation” and he felt no pain for about 2 hours, (2) the whole time of operation was less than 10 minutes, and (3) “there was not the slightest need for interference with the carotid artery, or even to place a finger on a spouting vessel” as “the patient could not have lost more than from 8 to 9 oz. (226 gram to 255 gram) of blood, no ligatures were required” . He was discharged within 14 days in a perfectly healthy condition.
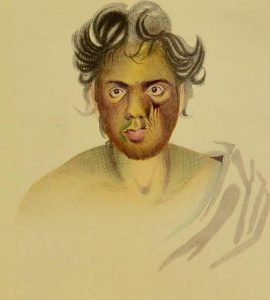
(Woodey (?Uday) Morrol after recovery – drawing by R O’Shaughnessy, December 1837. Courtesy: Wellcome Collection)
This was a great triumph of an institutional surgery for both the European surgeon and accurate European method of surgery on the one hand, and on the other, the surgery was meant for pedagogic purpose to inculcate European superiority among Indian students.
Here comes the question of functioning of CMC. Before going into its detail, which will be dealt with later on, some relevant issues can be discussed.
The original staff of the Calcutta Medical College consisted of a Supt., Assistant Surgeon M, J. Bramley, with Assistant Surgeon H. H. Goodeve as his only assistant. These officers were granted staff salaries of Rs.1200 and Rs.6oo respectively, in addition to the regimental pay and allowances of their rank; and had to devote their whole time to the College, not being allowed to practice. Bengal Civil Order No. 33. of 1st Feb., 1837, made the following appointments, Goodeve retaining the professorship of Medicine and Anatomy, and W. B. O’Shaughnessy that of Chemistry and Materia Medica.
Further additions to the staff strength of the College were such – Assistant Surgeon C. C. Egerton to be Professor of Surgery and Clinical Surgery, Surgeon N. Wallich, Supt. Botanical Gardens, to be Professor of Botany, Assistant Surgeon T. Chapman, to be Lecturer on Clinical Medicine, Assistant Surgeon J. McCosh to officiate as Lecturer on Clinical Medicine, Mr. R. O’Shaughnessy to be Demonstrator of Anatomy, Mr. David Hare to be Secretary. “McCosh resigned in the following year, 1838, when the lectureship on Clinical Medicine was abolished, and the salary saved devoted to the maintenance of a small clinical hospital, opened on ist April, 1838, to which an outpatient department was attached.”
It is evident from the above passage that when McCosh resigned from CMC his salary was used for the maintenance of the small clinical hospital attached to the College, not for a substitute faculty. It points to the fact that “economy of education” was most crucial to the profit-making EIC. What they did for education was basically to minimize expenses for bringing trained doctors from England. It will be more evident from an example of military training. A high-placed military official W. J Moore referred Colonel Hodgson to make it clear that “the British soldier who now serves in Bengal one year encounters as much risk of life as in three such battles as Waterloo.” Moreover, “The loss many hundreds of soldiers, each of whom has cost the state £100 to train to his duty, has resulted from the neglect of sanitary regulations, and it may be added, a long depreciation of the medical department.”
Moore brought two issues to the notice of the readers – (1) training of each soldier has cost the state £100, and it can presumably be avoided if the training is done in India, and (2) there was neglect of sanitary regulations leading longstanding depreciation of the medical department. Hence, sanitary principles and military training in India should be emphasized. In another document it was clearly stated – “Native surgeons, educated at the Company’s Medical College in Calcutta, could be easily procured, and would be glad to be employed, at from Rs 25 to Rs 50 per month, with rations and a free passage.”
Another account may seem interesting to us. “Passage-money to India, 8c.— If he should proceed in one of the Company’s ships, he will have to pay 95l. for his accommodation at the captain’s table, or 5l. for his accommodation at the third-mate’s mess” In 1835, a professor of CMC would get around £60 per month. So it was not easy for them to bear the cost of the journey frequently. Also the journey to England would take three months or more. As result, to stay in India for a long time was a better option for them.
Coming back Richard O’Shaughnessy’s complicated but utterly successful surgery, the surgery performed before the expectant eyes of the students led to far reaching implications. It helped in the creation of a new medical cosmology. Moreover, there occurred the complete epistemological rupture with the predominant and traditional knowledge systems (like Ayurveda). A new social psyche to assimilate the new knowledge was in the making. Briefly speaking, it led to a number of emerging characteristics.
First, when the students were acquiring knowledge in English and learning new medical terms and idioms of expression they came to associate themselves with a new kind of auditory as well as verbal acculturation. When they were exploring into the inside or the third dimension of the body it resulted in an altogether new visual acculturation. Learning how the bodily organs function through definite dynamics or hands-on training in chemistry classes bolstered this process. Gradually they became citizens of new epistemological praxis and medical cosmology as well.
Second, the new visual acculturation through dissection, surgery, post-mortem examinations and others was not only a kind of acculturation. More importantly, it remoulded “philosophy of observation” resulting in clinical gaze a la Foucault. “The space of configuration of the disease and the space of localization of the illness in the body have been superimposed, in medical experience, for only a relatively short period of time—the period that coincides with nineteenth-century medicine and the privileges accorded to pathological anatomy. This is the period that marks the suzerainty of the gaze.” Moreover, “The clinical gaze has the paradoxical ability to hear a language as soon as it perceives a spectacle. In the clinic, what is manifested is originally what is spoken.”
The students began to learn accurately the third dimension, instead of two-dimensional bodies which were graphically portrayed so far. The gaze extended from the surface to the interiors.
It should be stressed here that Foucault emphasized on two more issues – (1) “The hospital became viable for private initiative from the moment that sickness, which had come to seek a cure, was turned into a spectacle. Helping ended up by paying, thanks to the virtues of the clinical gaze” and (2) regarding the difference between the and the hospital – “the role of the hospital doctor is to discover the disease in the patient; and this interiority of the disease means that it is often buried in the patient, concealed within him like a cryptogram. In the clinic, on the other hand, one is dealing with diseases that happen to be afflicting this or that patient: what is present is the disease itself, in the body that is appropriate to it, which is not that of the patient, but that of its truth.”
What Foucault experienced in the French clinics and European hospital is not fully compatible in Indian perspective. Here the genesis of “hospital medicine” or the birth of the clinic did not historically evolve through social, economic and political changes. Rather it was engrafted on Indian specificity to suit British purpose. Only within a span of hardly two decades, the victory over European “hospital medicine” over millennial indigenous medical practices was practically settled. Indian milieu was not prepared for it. It was rather a kind of cultural shock.
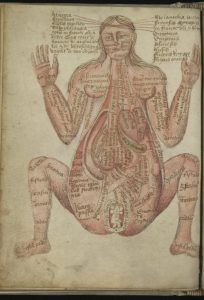
(A 15th Century Drawing of the Human body. Courtesy: https://publicdomainreview.org/collection/anatomical-illustrations-from-15th-century-england)
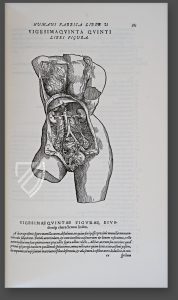
(A drawing by Vesalius, 1543. The body attains three-dimensionality)
To be precise, patient’s account of the disease (symptoms) lost its role. What the doctor found and extracted from his own examinations (signs) became the only truth.
Following Ackerknecht, “hospital medicine” developed in tandem with the onslaught of industrial revolution in Europe – “These were essentially a consequence of the tremendous influx of uprooted and penniless boys and girls from the country and of the beginnings of the Industrial Revolution.” Such idea is substantiated by other researchers too – “The patients were poor, less articulate, less troublesome, and it was much easier to carry out research on them (especially statistically based research which required large numbers in one place – the hospital). Moreover, the advantage of the poor was that the large numbers of post-mortems that were carried out would elicit no complaints from influential families.”
All these observations are a definite pointer to a social condition where economic changes are going, forcing people to become penniless and uprooted. A few more characteristics of hospital medicine which took a definite institutional shape in Parisian hospital may be elaborated. Earlier on, as a patient recounted how he or she fell ill, the story itself was the object of scrutiny by doctor and patient alike. Both were, in effect, able to hold the narrative up to the light and make of it what they would. “By the 1780s, the patient’s narrative was no longer the focus of inquiry in the infirmary.” Regarding teaching at a Paris hospital one American student described his experience, there were hundreds, nay thousands of individuals, employed in demonstrating, teaching, and unraveling, in every possible way, the most intricate subjects, in every branch of our science and art, and for a compensation so exceedingly small, and, oftentimes, without any compensation at all, as to be within the limits of the poorest and most destitute student. … Above all, I found that the regular lectures in the different hospitals and institutions, by men of the first eminence, were paid for by government, and gratuitous, as respected the pupil.
It is important to remember that the Parisian hospitals (unlike most of the English medical schools for anatomical teaching) were controlled by the government, which employed clinicians to attend patients and to teach, and, thus, “fostered the access of instructors and students to the bodies of living patients and their remains after death. By contrast, the London hospitals were private charitable institutions with lay boards of governors that vested medical control in a small number of socially elite physicians and surgeons.” Joan Lane reminds us that the changes in hospitals in the nineteenth century were in important areas like medical teaching, and the whole profession expanded as never before. The acute sick came to “outnumber the long-term chronic patients…the hospitals became more ‘medicalised’…” The French experience of the rise of hospital medicine heralded the closing hour of medical medievalism. It was no longer possible to practice without examination. “Surgeons, used to extirpating the lesions of the disease, and physicians, used to administering systemic medicaments, all suddenly now needed a blanket system that could unite heretofore disparate perspectives on the ‘seats and causes of disease’.”
We have come a long way treading the trajectory of the rise of hospital medicine and modern medical teaching hospitals in a very brief way. In early nineteenth century, Calcutta also followed somewhat similar pattern – “Every one (sic) knows that this city contains thousands of poor strangers, of all ranks, without wealth, connexion, or friends, who when afflicted with disease, fly from the city, and receiving medicine, and the prescribed regimen elsewhere, recover: but some die on the road, and many perish for want of two pice worth of medicine. Those who live from hand to mouth cannot obtain proper food or medicine, and for them there is no relief. Those who have no attendance, and no means of obtaining medicine, perish of course by hundreds in the city.” These poor, wretched of the earth, hapless people took their refuge in CMC before death, where they could at least get two or three full meals. During their living state they became the spectacle of diseases, and, after death, they became useful for dissection newly introduced in CMC. “Mortui vivis docent – the dead teach the living.”
The question arises – what were the phases before the advent of hospital? Medical historians have broadly classified them into two categories – “philosophical” or “scholastic” medicine and “bed side” medicine. Herman Boerhaave is the most illustrious figure of bedside medicine. He was most famous and esteemed to the extent that “it was said that he received promptly a letter from China, with the simple address “To Mr. Boerhaave in Europe.” Ackerknecht sharply differentiates between the new hospital and the medicine of Boerhaave – “The tweleve beds of Boerhaave’s clinic cannot be compared with the 20,341 persons residing in forty-eight Paris hospitals in 1784.”
Coming back to CMC, the students had to attend punctually regular classes at the College. So they had to follow the strict clock-time on the one hand, and provide systematic study of European medicine and provide answers to their questions more systematically. As a sum total, they had to attune themselves to a new kind discipline and governance very much needed for “modern citizenry” of the emerging modern state. They had also to be docile, disciplined and obedient. All these characteristics of a new kind of identity were naturalized in gradual process. This was sort of clock-time acculturation for the new generation of students and would-be citizens of India. Sumit Sarkar briefly describes the process in this way – “Disciplinary time was a particularly abrupt and imposed innovation in colonial India. Europe had gone through a much slower and phased transition spanning over some five hundred years … Colonial rule telescoped the entire process for India within one or two generations.”
According Jewson, the mode of production of medical knowledge was fundamentally transformed – “dramatic transformation in the form of medical cosmology occurred at the Parisian hospital schools during the first three or four decades of the 19th century with the introduction of a new mode of production of medical knowledge, here termed Hospital Medicine. The raw materials of medical theorizing now became the innumerable morbid events, occurring within the gross anatomical structures, which presented themselves to the clinical gaze on the crowded wards. Medical investigators concentrated upon the accurate diagnosis and classification of cases rather than upon the prognosis and therapy of symptom complexes.”
Such changes did not match anything or were not compatible in any way with pre-modern/pre-British Indian knowledge system. It was an altogether novel process. Hence the history of CMC is not confined within its walls at all – be in pedagogy, cultural milieu or epistemological praxis. It is deeply involved with the production of new knowledge system and new citizens (going beyond the realm of king-subject relationship).
Later on, with the foundation and expansion of dispensaries throughout India new techniques of governance penetrated deep into Indian social life too. If those people living beyond the space of modern governance could be brought under the surveillance of local dispensaries and made to learn the techniques of modern hygiene, sanitation and other health programs modern state could attain its viability.
Arnold has aptly said – “Medicine was thus seen to be more than liberation from disease. It was also viewed as a means by which Indian society might be liberated from its ignorance and superstition.”
Before its foundation as the first Asian medical college imparting modern European medical knowledge and training in European mode of teaching, CMC had a gestation period or period of nativity. It did not all on a sudden on Indian soil. Taking cue from Toby Gelfand regarding burgeoning clinics and hospitals in post-Revolution France, “background for the clinic’s nativity, a “gestation period”, which may add to our understanding of its lineage while preserving the notion of a sudden emergence.” Again, “the eighteenth-century surgical clinic served later medical reformers as a useful precedent. Its historical role in the “gestation” of the clinic helps explain why the new medical structure displayed certain specific and general characteristics.”
Here lies the importance of the NMI and medical classes at the Sanskrit College. Along with the foundation of the CMC they were abolished on the same day. The same G.O., by the authority of which CMC was established, clearly mentioned – “Govt. G.O. No. 28 of 28th Jan., 1835, The Right Honourable the Governor General of India in Council is pleased to pass the following resolutions. I. That the Sanskrit College medical class, the medical class Madrissa, and of the Native Medical Institution, be abolished from the 1st proximo.” This was the 1st resolution of 35 clauses related to the foundation of the CMC.
But the abolished institutions served the purpose of the “gestation period” or the period of nativity for the CMC.
References:
- Anonymous, “British Medicine in India”, British Medical Journal (hereafter BMJ) 1907, 1 (2421): 1245-1253.
- D. G. Crawford, A History of Indian Medical Service, in 2 volumes (Calcutta: 1914), Vol. 1, Chapters V and IX.
- Ibid, 37,
- Nicolao Manucci, Storia do Mogor, or Mogul India, 1653-1708, Vol. I, 219.
- Donald McDonald, Surgeons Twoe and A Barber (London: 1950), 30.
- Ibid, 30.
- Crawford, A History, Vol. 1, 53.
- Ibid, 54-55.
- Ibid, 57.
- Crawford, A History, Vol. 1, 113.
- Ibid, 113-114.
- Donald McDonald, “The Indian Medical Service. A Short Account of its Achievements 1600 — 1947”, Journal of the Royal Society of Medicine 1956, 49 (1): 13-17 (13).
- Crawford, A History, Vol. 1, 111.
- Ibid, 111.
- “British Medicine in India”, 1248-1249.
- Ibid, 1249.
- Crawford, A History, Vol. 1, 118.
- J. Talboys Wheeler, Early Records of British India: A History of the British Settlements in India, (London: 1878), 185.
- Eyre Chatterton, A History of the Church of England in India Since the Early Days of the East India Company, (London: 1923), 57.
- Alexander Hamilton, A New Account of the East Indies, Being the Observations and Remarks, Vol. II, (Edinburgh: 1727), 11.
- Revd. J. Long, Selections from Unpublished Records of Government for the Year 1748 to 1767…, Vol. 1, (Calcutta: 1869), 514.
- Ibid, 234-235.
- Ibid, 234.
- C. A. Bayly, Empire and Information. Intelligence Gathering and Social Communication in India, 178-1870, (South Asian Edition: 2017), 281.
- Charles Lushington, The History, Design and Present State of the Religious, Benevolent and Charitable Institutions, Founded by the British in Calcutta and Its Vicinity (Calcutta: 1824), 292.
- Harrison’s Principles of Internal Medicine, 19th edition, 2016, Vol. 1, 5
- Guenter B. Risse, Mending bodies, saving souls: a history of hospitals (New York: 1999), 623.
- D. G. Crawford, A History of Indian Medical Service, 1600-1913, in 2 volumes, Vol. 2 (Calcutta: 1914), 418.
- Ibid, 421.
- Ibid, 423.
- Ibid, 421.
- Ibid, 422.
- Ibid, 424.
- Ibid, 424.
- Ibid, 426.
- Ibid, 425.
- E. O’G. Kirwan, “Early Ophthalmologists in Calcutta”, British Journal of Ophthalmology 1937 Dec, 21 (12): 638-644.
- Crawford, A History, Vol. 2, 425.
- From Western Medicine to Global Medicine: The Hospital Beyond the West, ed. Mark Harrison, Margaret Jones and Helen Sweet (Delhi: 2009), 14.
- The Diaries of Streynsham Master 1675—1680 and Other Contemporary Papers, ed. Richard Carnac Temple (London: 1911), Vol. 1, 431.
- Arthur Broome, History of the Rise and Progress of Bengal Army (Calcutta: 1855), Vol. 1, Appendix R, U and W.
- Ibid, Appendix P, xxxi.
- D. G. Crawford, A History, Vol. II, 102.
- Ibid, 107.
- Ibid, p. 107.
- Charles Lushington, The History, Design, and Present State of the Religious, Benevolent and Charitable Institutions, Founded by the British in Calcutta (Calcutta: 1824), 312-13. [Emphasis added]
- Ibid, 313-14.
- Ibid, p. 314.
- Crawford, A History, Vol. 2, 96.
- Richard O’Shaughnessy, “Case of Enormous Tumour of the Upper Jaw”, The Quarterly Journal of the Calcutta Medical and Physical Society, January 1, 1838: 1-8.
- R. O’Shaughnessy, “Enormous Tumour of the Upper Jaw Successfully Removed by Operation”, Lancet 1838, 30 (768): 268-271. For the author, the journal introduced him as “R. O’Shaughnessy, Esq., M. R. C. S. Demonstrator of Anatomy, Medical College, Calcutta, and Superintendent of the Gurranhatta Dispensary”.
- Ibid, 270.
- [Owsei Temkin, “The Role of Surgery in the Rise of Modern Medical Thought:, Bulletin of the history of Medicine 1951, 25 (3): 248-259 (259).
- D. G. Crawford, A History of Indian Medical Service, 1600-1930, Vol. 2 (Calcutta, 1914), 435.
- Ibid, 436.
- O’Shaughnessy, “Case of Enormous Tumour of the Upper Jaw”, 3.
- Ibid, 3.
- Ibid, 4.
- Ibid, 5.
- Crawford, A History, Vol. 2, 438-439.
- W. J. Moore, Health in the tropics; or, sanitary art applied to Europeans in India (London: 1867), 13.
- Ibid, 6.
- Report of the Select Committee on Transportation; Together with the Minutes of Evidence, Appendix and Index, Appendix (B.) No. 34 (1838), 196. It was J. R Mayo’s testimony before the Select Committee on 22 June 1837.
- “Assistant Surgeons in the East India Company’s Service”, Lancet 9 July 1831, 16 (410): 477-478 (478).
- For insightful discussion on this issue, see, N. D. Jewson, “The disappearance of the sick-man from medical cosmology, 1770-1870”, International Journal of Epidemiology 2009 Jun, 38 (3):622-33.
- Michel Foucault, The Birth of the Clinic: An Archaeology of Medical Perception (Tavistock Publication: 1976), 3-4.
- Ibid, 108. (Emphasis in original)
- Foucault, idem, 85.
- Ibid, 59.
- For detailed discussion on hospital medicine, see the pioneering work of Erwin H. Ackerknecht, Medicine at the Paris Hospital, 1794-1848 (Baltimore: 1967) – “it was only at the hospital that the three pillars of the new medicine – physical examination, autopsy, and statistics – could be developed.” (p. 15)
- For insightful discussion on this topic, see, N. D. Jewson, “The Disappearance of the Sick-Man from Medical Cosmology, 1770-1870”, Sociology 1976, 10 (2), 225–244.
- Ackerknecht, idem, 15.
- Andrew Wear, “Introduction,” in Medicine in Society: Historical Essays, ed., Andrew Wear (Cambridge: 1998), 1-13 (6). [Emphasis added]
- Marry E. Fissel, “The disappearance of the patient’s narrative and the invention of hospital medicine,” in British Medicine in an Age of Reform, eds., Roger French and Andrew Wear (London, New York: Routledge, 1991), 92-109 (99).
- John Harley Warner, “Paradigm Lost or Paradise Declining? American Physicians and the ‘Dead End’ of the Paris Clinical School,” in Constructing Paris Medicine, eds., Caroline Hanaway and Ann La Berge (Amsterdam: 1999), 337-383 (344).
- Ibid, p. 343.
- Joan Lane, A Social History of Medicine: Health, healing and disease in England, 1750-1950 (London: 2001), 87.
- Russel C. Maulitz, “The pathological tradition,” in Companion Encyclopedia of the History of Medicine, W. F. Bynum and Roy Porter (ed.), vol. I (London: 1993), 169-191 (178).
- James Peggs, India’s Cries to British Humanity… (London: 1832), 203. Emphasis in original.
- Andrew Cunningham, “The kinds of anatomy”, Medical History 1975, 19 (1): 1-19. Also see, L.S. King and M. C. Mehan, “A History of Autopsy. A Review”, American Journal of Pathology 1973, 73 (2): 514-544.
- Arturo Castiglioni, A History of Medicine (New York: 1947), 615.
- Ackerknecht, Medicine at the Paris Hospital, 15.
- Sumit Sarkar, Writing Social History (New Delhi: 2002), 309.
- Jewson, “The disappearance of the sick-man”, 624.
- David Arnold, Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth-Century India (Berkeley: 1993), 58.
- Toby Gelfand, “Gestation of the Clinic”, Medical History 1981, 25: 169-180 (170).
- Ibid, 180.
- Crawford, A History, Vol. 2, 435.








