

Preliminary Remarks
As we shall see later, in the entire report of 1842-43, besides dissection, details of classes, different subjects taught in the College and Hospital, hospital management, there was also mention of “Museum” and “Library”. But there was no mention of any laboratory activities at all. Even the name of any laboratory at the College, though we have earlier come across of providing microscope to the students, was glaringly absent. Cogently one can ask why laboratory was so conspicuous by its absence in the Report.
From the 1830s medicine entered into the era of “laboratory medicine” – more experimental in nature with heavy gradient to the understanding of physiological processes. At the CMC, W. B. O’Shaugnessy started this exercises in his classes during 1836 to 1839. But later the spirit of experimentation dwindled and, finally, almost disappeared. Pedagogy of the College was happy with dissection-based pathological anatomy. In this way, the teaching in the CMC was far away from developments in Germany, France, England and America.
The Germans created institutes in all the medical sciences, the most notable one in physiology being that of Carl Ludwig (1816–95) at the University of Leipzig, where students from all over the world trained. Ludwig was one of a group of four young physiologists who during the revolutionary year 1848 issued a manifesto, declaring that all the problems of physiology could be solved by the systematic application of physics and chemistry. Two of the others in the group went on to head physiology institutes in Berlin and Vienna, and the fourth, Hermann von Helmholtz, eventually turned to physics. In addition to important work in electromagnetism and conservation of energy, he was an expert in the physiology of the special sense organs, and the physics of hearing. All four of the group maintained their basic physical orientation to physiology.
The laboratories of these and other German physiologists began to acquire a modern look, as scientists availed themselves of the latest technological aids. Helmholtz invented the ophthalmoscope, and Ludwig developed the kymograph, a turning drum connected to a recording device that allowed the measurement of continuous functional variations, such as the pulse, muscle contractions, or changes in tension. The graphical recording of vital events has increasingly characterized biomedical research and clinical medicine. Physiology flourished in Germany, although the pre-eminent physiologist of the century was French: Claude Bernard (1813–78). He went through the Paris medical school, and recognized that the clinical orientation that dominated it could only go so far in understanding disease mechanisms or in searching for new remedies.[1]
It has been shown by Roy Porter, the celebrated historian of medicine, “Physiology came of age as a high-status experimental discipline. Its trailblazer was Johannes Müller, from 1833 professor of physiology and anatomy at Berlin. His enormous Handbook of Physiology (two volumes, 1833–40) served for many years as the bible of the discipline.”[2] The four most famous students of Muller were Theodor Schwann, Hermann von Helmholtz, Emil du Bois-Reymond and Karl Ludwig. According to Ludwig, “there could be no medicine without physiology, since ‘every case of illness is a physiological experiment … and each physiological experiment is an artificially produced illness.”[3] It was further emphasized by Claude Bernard, “A physiological laboratory, therefore, should now be the culminating goal of any scientific physician’s studies; but here again I must explain myself to avoid misunderstanding. Hospitals, or rather hospital wards, are not physicians’ laboratories, as is often believed”[4].
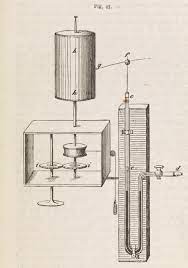
(Kymograph of Ludwig – Wikimedia)

(Stromuhr – to measure arterial blood flow – London Museum)
One researcher has observed, “Just ahead was a pedagogical revolution in medical teaching – the rise and spread of laboratory teaching – that would add still further to the burdens of future students of medicine.”[5] He further notes that no one questioned the advantages afforded by the new chemistry and physics to those who used them in research in a special workplace, now called the laboratory, but the “belief that practical experience [in a laboratory] was important for all students, not merely for a small elite” constituted the real pedagogical revolution in the teaching of medicine. Like the earlier shift to clinical teaching, the transition to laboratory teaching, including the use of the microscope, came slowly and sporadically, had roots in the immediate past, was justified by its practical uses, and was shaped by a variety of educational and political circumstances in each country.[6] It started robustly in Germany in the 1830s and spread then to other Euro-American countries.
Unfortunately, in 1840s and, also later on for quite some time, CMC was confined within the cocoon of ‘hospital medicine’ – post-mortem dissection and clinical teaching, but not any laboratory-centred physiological researches – failing to transcend into the higher level of scientific studies and experimentation. Most likely, the primary cause was that colonial authorities wanted only capable practitioners for their daily chores of medical requirement, but not capable practitioners as well as capable enquirers at all. Most likely it happened that medical education at CMC was shaped by a variety of educational and political circumstances in each country – in India it was undoubtedly was colonial interest.
General Reports Related to the CMC
We have seen previously in the GCPI (1839) that as the first four students – Umacharan Set, Rajkrishna Dey, Dwarakanath Gupta and Nobin Chnardra Mitra, to whom Shyama Charan Dutta was later included – did not complete the period of study of minimum four years, they were not awarded the degree of Graduate of Bengal Medical College (GBMC). Rather they were awarded with “letters testimonial” title. H. T. Prinsep, Secretary to the Government of Inida, while making an evaluation of CMC before, during and after the first qualifying examination wrote to the General Committee of Public Instruction on 5 December, 1838, “who appeared before us on the 30th October … at the end of six months’ probation to which we remanded two of them, and which others of their own accord fell back upon, may become candidates again for letters testimonial”[7].
Moreover, “Should these young men be appointed immediately to dispensaries, or any other medical charge … They should always keep regular case books as records of their practice with house patients.”[8] It appears form later reports that more students passed and were entrusted with duties of dispensaries which were spread throughout distant of parts of the North-Western Provinces, established in 1836, through merging the administrative divisions of the Ceded and Conquered Provinces, and Bengal.
Report of the 5th year (“for the year 1839-40”) informs us, “An additional class has been formed for the purpose of educating Native Doctors for the employment in the Army.”[9] It was also clearly mentioned that such body of servants was much needed and it completely ceased after the “abolition of Dr. Tytler’s Native Medical School”[10]. Basically it came out as an endeavour of W. B. O’Shaughnessy to train and teach in vernaculars (training in native languages) and, most interestingly, it was conceived within the womb of the CMC, fully guided by European medical training. Thus the trace of Orientalist history could keep its imprint on Anglicist version of history. This secondary school was constituted by “His Honor, the President in Council, dated 12th August, 1839.”[11] In the month of October 50 students “were selected, from a very large assemblage of young men. Upwards of twenty more remained on the list, as expectants, to be admitted as vacancies occurred.”[12] Again, some kind of selection process was inevitable, which later through many evolutions and developments metamorphose into our present day entrance examinations.
For this Secondary class, to instruct the new pupils three teachers were chosen from among the English class. They were “Sib Chuinder Kurmacar, Chimunlall, and Navakrishna Goopto … The instruction differs from that of Dr. Tytler, as in much as the subjects are taught practically, by the aid of the Dissecting Room, Laboratory, and Hospital.”[13] These pupils were primarily taught for filling in the vacancies in army at various stations.
The report states that “A large Female Hospital, intended to embrace the advantages of a Lying-in-Hospital with instruction Midwifery, has been commenced, and is now ready to receive patients.”[14] It had the capacity of accommodating more than hundred patients. The Male Hospital, opened in April 1839, continued to receive “an abundant supply of patients of all classes, Europeans, as well as Natives … The readiness with which natives of every caste from the Brahmin downwards … without objection to the religion or caste of any of the other occupants of the same ward, or even of the next beds, offers a convincing proof of the little necessity which exists, in similar Institutions, for separating the native patients from each other, on account of religious prejudices.”[15] There was a separate group of European patients who “were transferred to the College from the Police Hospital”[16].
Accommodating different kinds of patients in the college hospital provided an excellent means of clinical instructions to the students. There was dispensary attached to the college hospital – open from 6 to 10 A. M. and 4 to 6 P. M. and daily receiving 200 to 300 students for treatment.[17] In this session, there were 41 students on the foundation list, and 38 free students of various religions. There were also students from families of the European and Armenian inhabitants of the city “showing that the advantages of the College are gradually extending themselves to the community at large … as a part of the Educational Establishment of the country.”[18]
Some thoughts on the Beginning of Public Health in Colonial India
Nine of the passed out students were employed in the dispensaries at Delhi, Agra, Allahabad, ‘Cawnpur’, Bareilly, Benares, ‘Moorshedabad’, Assam and Meerut. It was mentioned, “It is recorded that many dispensaries were at this time opened in various parts of the Province, supported partly by the Government and partly by private subscription. These were placed under the charge of Sub-Assistant Surgeons passed from the newly formed Medical College, and under the immediate superintendence of Civil Surgeons.”[19] To my analysis, it was the kernel of a definite program on public health for the first time in colonial India – in its conception, structure, manning and penetration to the interiors of the Indian society. It was clearly stated that the “General Committee learned with much pleasure the success of the Dispensaries which have been placed under the charge of the Sub-Assistant Surgeons, and they trust, that the system will be further gradually extended as pupils are fitted for employment.”[20] The report went on – “The number of patients treated, and the success of the practice is highly satisfactory. A number of operations were also performed by them with success, so that the Sub-Assistant Surgeons may be considered as capable of coping with all the usual exigencies of the profession.”[21]
My conception of the origin of public health in colonial India does not conform to the ideas of the celebrated and esteemed historians like David Arnold or Mark Harrison. Rather it contradicts their ideas. According to Arnold, “arguably, the moment of transition from enclavism to public health came only in the 1890s with the establishment of a new “tropical medicine,” based on the germ theory of disease, and a corresponding intensification in state medical intervention in India as in many other parts of the colonial world, epitomized by the measures taken during the Indian plague epidemic of the 1890s and 1900s.”[22] Elsewhere, Arnold argues that IMS officers were employed in a wide range of civilian as well as military duties: they ran hospitals, supervised jails, and presided over provincial sanitation and vaccination departments. In times of war, however, the army’s needs took priority and IMS officers were drafted back to military duties. This military nexus had far-reaching consequences for the nature of state medicine and public health in India. For much of the 19th century the army (supplemented by the jails) was the primary site of clinical observation and main source of medical statistics.[23]
Arnold also contends that “Even if the reach and efficacy of Western medicine was strictly limited in the period up to the 1860s and, as Radhika Ramasubban contends, barely extended beyond a small European enclave, it was nonetheless important in laying the foundation for later developments and in establishing the claims of Western medicine, and of Western authority more generally, over India and its colonial subjects.”[24]
In Mark Harrison’s argument, The history of public health administration in India also dates from the assumption of Crown rule. In 1859, in the wake of the mutiny, a special commission was set up to inquire into the sanitary state of the British Army in India. Epidemic disease had seriously depleted the fighting capacity of British troops in 1857, and, in the light of the public outcry over preventable deaths in the Crimea, there was increasing concern in Britain over military hygiene in India.[25]
To put the crooked historical facts in a simpler way, in our analysis, there were three stages in the beginning and development of public health in colonial India – (1) military medical teaching at the Native Medical Institution (NMI) and deployment of its students among the Indian community during the outbreak of cholera, which led to the early genesis of public health issues, (2) transition from military medical training to universal, civilian and general European medical education at the CMC without religious, social status or caste bar, and (3) deployment of CMC passed outs to various dispensaries to take care of general populace at large.
When the cholera epidemic struck Calcutta in the 1820s, twenty of Breton’s (the then superintendent of the NMI) “most experienced pupils” were dispatched among the local population with the hope that a “decrease in the number of cases of cholera in the town will now admit of the aid” of his students.[26] In a letter to Dr Breton, Radhakanta Deb wrote, “I shall introduce and recommend your advice and medicine, both here and in the interior; and the human lives which will thereby be saved.”[27] Thus the background for the gestation of public health in India was prepared. Western education became successful in producing its agency through elite people like Radhakanta. We shall shortly come to know how these rudimentary beginnings took definite shape through the expansion of dispensaries.
Later on, deployment of the pass outs and manning various dispensaries in different corners of India, as we shall below, gave the much needed strength to a full scale functioning of public health in India. It was not journey from ‘enclavism’ to public health through the tortuous route to battle with epidemics, But it goes without saying that the flourishing of public health in colonial India and demonstration of its grit, strength and weakness were definitely fully tested in the times epidemics, when full scale mobilization of public health activities was done to save primarily the military and new recruits of the army. Even the protection of Indian population in the times of epidemic was also a big issue under the scrutiny of international sanitary experts.
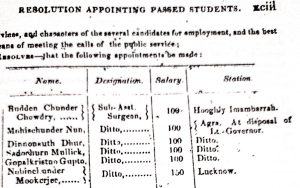
Below is a list of students who were appointed in various dispensaries just after passing out from College.[28]
In 1847, Balfour felt that perhaps one of the most striking features of the present history of India was the wonderful success with the opening of Dispensaries.[29] Moreover, The branch dispensaries would, it was conceived, bring fair medical aid within the reach of many who were at present utterly deprived of it; would be a means of saving life and preserving health to the police, and such of the inhabitants of the Terace as choose to apply; would secure a fair union in the instance of broken bones , sword cuts and common injuries: and, with regard to the more serious surgical cases, might act as feeders to the central dispensary (for it was never contemplated that the great operations should be performed within:) and it was supposed that from thirty to fifty patients a day might be expected , on the average … I have also discouraged application for advice from the sick directly made to myself, requesting them to apply to the native doctor in the first instance, and consulting with him afterwards, if required by the severity of the case.[30]
Dispensaries, in his view, were held by the great majority of the people with increasing favour. They were manned by graduate sub-assistant surgeons of the CMC. Thus, it was through the dispensary that a space for modern public health was opened up in a true sense. The success of these strategies was also dependent on the internalization of certain rules of behaviour by the population at large. “Medicine thus acquired political status inasmuch as it gained a new relevance to the interests of the state”.[31] Taking stock of some of the dispensaries of Northern India, Sykes observes, “Confining myself to the broad features, I may state, that 267,456 cases including house and outpatients, were treated – of this number 168, 871 were cured, 2417 died, and 96,168 ceased to attend”[32]. We have to keep in mind that these figures represent only statistics from the Northern part of India. If one added figures from the North-Western provinces and Bengal this statistics must show a greater number of patients to being benefited by dispensary services. The crux of public health question – bringing a great number of populace under the cover of modern medical treatment – was thus resolved at the outset.
Coming Back to the Annual Reports of the CMC
It should also be noted that several of the passed out students of the first five years did not enter into the government service. Dwarakanath Gupta had established himself in extensive practice in Calcutta (now Kolkata). Moreover, he was a head partner in a well conducted and flourishing apothecary’s establishment. Ramkumar Dutta and Gobindachandra Gupta had also successfully established themselves as practitioners and apothecaries in Calcutta. We can deduce that these early stalwarts from CMC heralded the beginning of private practice on the one hand, and drug store on the other. It was reported – “These establishments are calculated to prove of great public benefit by reducing the cost of the drugs used in the practice of medicine to the means of the larger classes of the community who, from the consideration of economy, were hitherto compelled to use the cheap nostrums and poisons of the Bazar.”[33]
Nabinchandra Mukherjee was employed by the Assam Tea Company on a salary of Rs. 150 per month. Shibchandra Karmakar and Navakrishna Gupta were employed as teachers in the Secondary School of CMC. Nabinchandra Mitra was in charge of the College out-door dispensary. Gopal Krishna Gupta had returned from his private service in Assam owing to ill health.[34] In a sense, as we shall come to see, through the establishment dispensaries and their successful operations “Bengali colonization” of different parts of India began to ensue. Regarding the sub-assistant surgeons it is learnt from the Report – “as almost all of them are natives of Bengal, and consequently strangers both in point of customs and language to the people of the Western Provinces, among whom many of them are appointed to labour, sometime must be allowed for the for the softening down of mutual prejudices.”[35] If we carefully look at the last sentence it seems to be a replica of British colonization of India.
Let us now do a quick survey of the dispensaries manned by the graduates of CMC. (1) Dacca – sub-assistant surgeon Nabin Chandra Pal, in-patients 23 (of these 16 were cured and 3 died), number of out-patients 2005. (2) Chittagang – sub-assistant surgeon Rajkrishna Chatterjee. (3) ‘Pooree Dispensary and Pilgrim Hospital’ – sub-assistant surgeon Nilmani Dutta – a in a span of six months 418 cases of principally fevers, bowel complaints and ulcers of various kinds were admitted . (4) ‘Moorshedabad’ – sub-assistant surgeon Panchanan Shrimoni – no capital operations were performed, some country medicines like ‘Kala Dana’ and ‘Kut Kelija’ were introduced into use. (5) Patna – sub-assistant surgeon Ram Ishwar Awasthi – out-patients 5492, of which 3320 were cured and 1803 ceased to attend, average daily number of sick 306. (6) Benares City Hospital & Secrole Dispensary – sub-assistant surgeon Ishan Chandra Ganguli – number of out-patients 3833. “Two apprentices have been attached to the Secrole Dispensary during 1837 and 1839, respectively. The elder, Jhammar, is a steady lad, but the younger, Bhandie Doss, gives some trouble.”[36] (7) Allahabad Dispensary – sub-assistant surgeon Shyamacharan Dutta – quite good number of surgeries done – 1 of amputation of the leg, 1 of the penis, 6 for cataract, 3 for fistula in ano, 1 for fistula in pereneo, 8 paracentesis abdominis, 8 for ectropian, and 2 for the removal of encysted tumours. Keeping in mind that it was pre-anaesthetic era and sans modern cutting-edge equipments, the number of surgeries done in such a dispensary was no doubt laudable and must have drawn respect from local population. (8) Bareilly Dispensary – sub-assistant surgeon Jadab Chandra Seth – out-patients 3062. It was reported that Jadab Chandra Seth through his skill and efficiency “have excited jealousy of the Hakeems, who do all in their power to thwart him, but prudence on his part and time will no doubt overcome their opposition.”[37] (9) Agra Dispensary – sub-assistant surgeon Uma Charan Seth – number of out-patients 3490 and average daily number of applicants 307 – quite a good number even in today’s respect.
From Jadab Chandra Seth’s activities and fierce opposition from traditional practices of Hakeems it transpires that there was a lingering epistemological struggle between two systems of knowledge – European and indigenous. At a much later date, this question was again dealt with in the Indian Medical Gazette.
On perusing lately the census returns of the North-Western Provinces, we were deeply interested, and strongly impressed, by that part of the returns which gave information as to the number of hakeems and baeds in the different districts of that Government. From this we gather that there are 7,000 practitioners of medicine and surgery in that division of the country, giving a proportion of one medical man to every 4,285 of the general population.
This is quite irrespective of Government employees, who are European Officers, supplemented and assisted by Sub-Assist- ant Surgeons and Native Doctors educated entirely on the European system, These, taken together, are, comparatively speaking, very few in number, and widely separated in their medical creed and practice from the baeds and hakeems (Vaidyas and Hakeems), with whom they have the least possible intercourse and sympathy … Under British rule, however, they have disappeared altogether from political life, and socially have little or no standing in European society, where they are virtually ignored.[38]
Moreover, it was anxiously noted, “In native society, all over the country, these men still hold their own, and are greatly respected, ministering as they do to the troubles of both body and mind of the people, and generally possessed of a superior education.”[39]
In the 8th year’s report (1842-43) of the CMC, which was placed on 30th April, 1843, we come to learn a lot about its developments, consolidation and ramifications through various tributaries.
We find the names of a number of Indians who were entrusted with different teaching areas. They were – Madhusudan Gupta, “Pundit” (salary 100 rupees per month), Navakrishna Gupta, “Teacher Secondary School” (same salary), Shbi Chandra Karmakar, “Teacher Secondary School” (of the same salary), Nabinchandra Mitra, “Apothecary Out-Door Dispensary (of the same salary) and Prasanna Kumar Mitra, “Resident Surgeon” (salary 50 rupees per month).[40]
It should be mentioned here that Navakrishna Gupta was previously doing his job in the small hospital attached to the Sanskrit College. He “was apparently doing quite well in that position at the hospital.”[41] Though dissection was never done in the Sanskrit College and major surgeries were beyond the scope of this institution, they “performed the dissection of the softer parts of animals”, and opened “little abscesses and dressing sores and cuts”.[42]
From the previous report (GRPI, 1842-43), we come to know that on the 12th day of the final examination a special section was on “Practical and Surgical Anatomy and Demonstrations of the Dead body”. “Each of the candidates dissected and demonstrated a region of the body and performed an operation … neatly executed, their demonstrations accurate.”[43] Two students were not qualified for “obtaining letters testimonial”.[44] Many modifications were done in the buildings of the College primarily for the surveillance of the students – a kind of Benthamite panopticon we might say – “the pupils from being located without the walls, not being sufficiently under control and personal superintendence of the college authorities.”[45]
The new structures will all be enclosed within the walls of the college compound, for which purpose the Civil Architect has been directed to negotiate for the purchase of certain adjacent huts, and portions of ground and roadway, with a view to the enclosure of that part of the old way, which at present separates the college premises from those occupied by the pupils from Ceylon, for whom a separate commodious building has been planned, capable of containing with comfort twenty-two individuals … The Library has been removed to the large room beneath the dissecting department, and is used for the monthly meetings of the Section of Council of Education for the medical College, and for holding all the viva voce public examinations.[46]
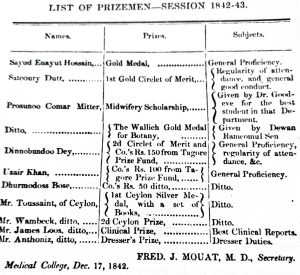
In this session, for the first the first time, “the Circlets of Merit” was awarded to the students showing excellence in their studies. Auckland, prior to his departure from India, provided two prizes for the outstanding students – one “handsome Compound Microscope” and the other “a similar instrument of less value.” Satkaree Dutta, after a searching trial, was given the first prize, while Mr. Ondaatje, a Sinhalese student, obtained the second prize. Ramkamal Sen, Dewan of the Bank of Bengal, gave a gold medal as prize to the best student for the three successive sessions.[47]
It was noted in the report that professor Goodeve received great help from Satkaree Dutta and Mr. Krickenbeck “in preparing dissections, in some cases of a complicated and minute nature.” The voluntary and gratuitous aid of Prasanna Kumar Mitra as well as Madhusudan Gupta – “the native teacher” – in assisting to instruct the pupils in the dissecting was also greatly appreciated. With a regretful note, it was reported that “The want of an adequate supply of dissecting instruments for the increasing extent of the anatomical class, was also mentioned by the Professor, but will not, it is hoped, be in future a drawback to this department.”[48] It was also reported that “Mr. O’Shaughnessy brought prominently to the notice of the College Council, the subject of the paucity of instruments allowed for dissection, which he declares to be to be quite inadequate to the wants of the class, and with which it is utterly impossible for many of them to become really good or neat dissectors.”[49]
From the above discussion a few issues become quite evident – (1) senior students of the institution were teaching the juniors, (2) Indian instructors were successfully replacing the British one, and (3) anatomical teaching, especially dissection, had spread to such an extent and taken such a big shape that dissecting instruments used so far from the beginning of the College were inadequate for effectively furthering the classes of anatomical dissections.
It was ascertained that most of the old instruments previously supplied had been worn out, broken or lost. As a remedy, to prevent “the occurrence of neglect, the Council of Education sanctioned a deposit of two Rupees from each of the dissecting student, from which any deficiency, not caused fair wear and tear, is to be made good.”[50] In one sense, it is also a historical phenomenon because of the fact that in 1836, when the first dissection was done, the students had gone through various processes of acculturations like visual, verbal, psychic, moral and others to prepare their minds for dissection and there was a great deal of anxiety among the teachers of the College and the British authorities as well. As a consequence, the names of the first four dissecting sting students could not be made public lest they become ostracized in society. But within a span of 6 years all these fears were wiped out. Dissection had assumed social legitimacy both within and outside the College. As a result of which the Council was confident enough to order a deposit of two rupees from every student before doing dissection. To mention, Rustomjee Cowasjee, a very rich Parsi of Bengal and owned ship building company, bank, insurance companies and others, donated “a sum of Company’s Rupees 600, to be devoted annually to the purchase of a Gold Medal, for the most proficient student in practical Anatomy.”[51]
As a special note, “The Midwifery ward continued to prosper, was always full of patients, and presented to the students of a variety of instructive cases, amongst women of all religions and nations … Prosunno Coomar Mitter, who as resident surgeon of the hospital, had fully attained the high character he bore as a student.”[52] It is interesting to note here that the question of institutional childbirth erased all barriers of caste, religion and different national identities. Moreover, for the time, we find the mention of resident surgeon of hospital.
In this session, it was the “first occasion on which any of the students from Ceylon, upon the prescribed terms, passed their final examination, and was presented with the certificate of qualification”[53]. This session also saw “Baboo Doorgachurn Bonerjee, late Head Master of Hare’s School, and Ganindramohan Tagore, a distinguished pupil, and scholar of the Hindoo College, and son Baboo Prosunnocoomar Tagore, together with the Apothecary to the General Hospital, were attending the delivered in the College”[54]. It afforded “a gratifying proof of the estimation in which the institution, and the branches of science taught within its walls, are beginning to be held among the members of the native community … who have not enjoyed the benefits of a professional education in Europe”[55].
For military class, it was noted in the report, “In consequence of certain irregularities committed in the neighbourhood, by the idle and evil disposed, after a careful examination of the offenders, ten were recommended to Government for expulsion, which was carried into effect, and has been attended with the best results, not a single complaint having since been made by the neighbouring inhabitants of misconduct on the part of the students, while their demeanour within the College has been quiet, orderly, and free from objection.”[56]
At the end of the session a good number students were found qualified to awarded with different prizes.
Mr. George Daly, the Apothecary to the institution, was possibly the first “House Surgeon to the Male Hospital”.[57] The New Code of Rules and Regulations” were prepared, which was later published first in 1844 and then in 1849.[58] In the new code, the category of “Free Students” was specifically explained – “The number of students wishing to obtain a complete medical at their own expense, shall be unlimited … The free students shall be subject to the same rules and regulations as the other pupils of the college, in all matters of discipline.”[59]
Regarding dispensaries, it was mentioned in the 1842-43 Report that sub-assistant surgeons “educated in the College, perform their duties, and the amount of good which has already resulted from their exertions … will add to the intrinsic value of the Dispensaries, which are so well adapted by their internal economy to obtain the confidence of the native inhabitants.”[60] Thus these dispensaries became the nidus of the future public health system in colonial India. What benefits did people get from the dispensary services? (1) “Many have their sight restored”, (2) “others have been cured of hydrocele and relieved when in the last stage of dropsy”, (3) “some have also derived effectual relief from the successful operation for ‘stone in the bladder’”, (4) “a few have been saved from a miserable death by amputation of diseased members” (in many cases cancerous), and (5) “large tumors have been removed.”[61]
It was observed that such operations “could not have been achieved by native practitioners without producing an impression on the minds of the most apathetic natives, and they must tend to spread far and wide the value of the Government Dispensaries.” Country medicines were generally used in each of those dispensaries, where their application was deemed proper and sufficient.[62]
In this report we find new entries of dispensaries both within and outside Calcutta – (1) Bhowanipore Dispensary, sub-assistant surgeon Kalachand Dey, (2) Chittagong Dispensary, sub-assistant surgeon Raj Krishna Chatterjee, (3) Cawnpore Dispensary, sub-assistant surgeon Ramnarayan Das, (4) Furruckabad Dispensary, sub-assistant surgeon Sadhu Charan Mallik, (5) Agra Dispensary, sub-assistant surgeon Umacharan Seth.[63]
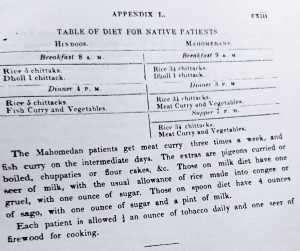
Definite rules or codifications regarding every details of classes, mode of teaching, students demeanour, hospital management, diets of patients and other paraphernalia were clearly stated, which was, as I have mentioned earlier, published as the book Rules and Regulations of the Bengal Medical College (1844, 1849). Regarding the Medical Hospital” it was written, The hospital attached to the Medical College is divided between the Professors of Surgery and Medicine. It consists of 3 wards capable of holding from 28 to 30 beds each, and two passages of 12 feet wide between the wards, capable of holding on an emergency from 14 to 16 beds, in all 112 beds. One ward is given up entirely to each Professor for the reception of native medical and surgical cases, and the other for the European patients is divided between them, but as the greater portion of the cases are purely medical, the students have innumerable opportunities of studying the effects of disease on the European constitution.
The hospital is open for the reception of all Europeans laboring under either severe medical disease or injury, who may apply for relief, or who are sent in by the Police. The patients are all dieted according to the annexed diet roll, and the charge for the diet of each patient is calculated for Europeans at 4 annas, and for natives 1 anna per diem.[64]
It becomes apparent from the allocation of funds for diet plan that there was glaringly racial discrimination existing among the Europeans and the Indians. Moreover, it was candidly accommodated in the directives related to hospital management.

Below is given the meagre amount of diet allocated for Indian patients.[65] These disparities were not consistent with the secularity practiced in the class room during teaching. While it was put against a more objective condition the discrimination became quite glaring.
Moreover, at later period, this kind of racial was categorically pronounced in hospital words too. In a different note, a general register of all the cases admitted in hospital “shall be kept, and available for statistical purposes”.[66] As an outcome of these rituals and procedures the ‘person’ of the patient began to disappear and, in turn, began to be known as a number: “Enter and you will find East Indians and West Indians, Bengalees and Madrasees…they are of all classes; and (as all patients are distinguished not by name, but by numbers), were one to ask for “Now Number Sahib”…”.[67] It must be noted here that as soon as a sick person entered a hospital ward he got transformed into an altogether different role of the patient. He becomes the receptacle of faulty pathology, chemistry and physiology as well. His reality is not compatible with the reality of the hospital ward. Though his body was carefully taken care of by the doctor, his sufferings remain unheeded. The doctor is the only tenuous link between the patient and his persona submerged within him.
The significant exception in the secular nature of the new medicine was determined by its colonial context where differences were often noted by caste and racial inscription.
Then, in the GRPI (1842-43), were reported every details of all the classes and how these classes would be arranged – in a definite order. It started with “Anatomy”, where it was stated – “The number of cases allowed for the dissecting class, shall be in the ratio of one case for every two students; the department being furnished in addition with three cases, for the teachers, a second-hand capital case for exhibiting all operations on the dead subject, a post mortem case, and such a number of spare saws, injecting syringes, &c ., as may be required”[68].
Next came “Demonstrations and Dissections”, followed by “Chemistry”, “Botany”, “Principles and Practice of Medicine”, “Surgery and Minor Surgery”, “Midwifery”, “Materia Medica and Therapeutics”, “Medical Hospital”, “Surgical Hospital”, “Female Hospital” and so on.
Under the section “Principles and Practice of Medicine”, definite objective was stated – “A complete course of lectures on the Theory and Practice of Medicine shall be given annually to the students of the Medical College of the 3rd and 4th year’s standing … In this course the general history of each disease shall be given, the pathology and plan of treatment fully entered upon, and the lectures illustrated, as much as possible, by cases that have occurred in the hospital.”[69]
In a similar way, under the section “Midwifery” the teaching plan was stated thus – “These lectures shall embrace a description of the female organs of generation, with their physiology, an account of the phenomena of labour, natural and preternatural, with the operations of Midwifery, the diseases belonging to the pregnant state and to women after delivery; the management of the mother and child during and after delivery: the diseases infants, and those belonging to the female system connected with pregnancy.”[70] It appears from this mode of teaching that the discipline of paediatrics was then submerged under the umbrella of midwifery. Paediatrics as a special subject was not in the offing.
To repeat what was mentioned earlier, under the section “Medical Hospital” it was made clear that The hospital attached to the Medical College is divided between the Professors of Surgery and Medicine. It consists of 3 wards capable of holding from 28 to 30 beds each … One ward is given up entirely to each Professor for the reception of native medical and surgical cases, and the other for the European patients is divided between them … The patients are all dieted according to the annexed diet roll, and the charge for the diet of each patient is calculated for Europeans at 4 annas, and for natives 1 anna per diem.[71]
We can note how materially racial discrimination with regard to the diet plan was so much obvious. Again under the same section –
On the admission of a patient into hospital he his sent to bed, has his clothes removed which are taken care of, and he has a hospital dress of clean linen put on. He is immediately seen by the Apothecary, who in cases of emergency prescribes, or otherwise waits until the daily visit of the Professor, which takes place at one o’clock, when the plan of treatment is laid down. The disease is noted on a ticket with the diet, date of admission, &c. spelling … The native patients and the European receive the same degree of attention. The Hospital at time is occupied with people of every race and caste, Hindoos, Musselmen, Jews, sometimes Armenian, French, Portuguese, and English.[72]
It is interesting to note that (1) in the management of hospital and some privileges provided to the patients ‘racial discrimination’ was apparent, but when it came under the ‘gaze’ of medicine the native patients and the European received the same degree of attention, and (2) how many nationalities of the world resided in Calcutta at that time – Hindus, Muslims, Jews, Armenians, French, Portuguese and English, most likely to name a few.
Further, under the same section, how the entire journey of ‘hospital medicine’ came to fruition was made evident – (1) bedside clinical teaching, (2) autopsy/post-mortem examination, and (3) statistics gathering –
Each student is shewn how to conduct an examination so as to form his diagnosis, and he is questioned as to the plan of treatment, and why he proposes such and such a course. The chief symptoms from diagnosis in each case are pointed out, and the several varieties of any one disease occurring in hospital … When the case terminates fatally the body will be examined by the Clinical Clerk before the Professor, the morbid changes noted, and the subject will be taken into the lecture room, and shewn to the assembled pupils, who will have the opportunity of observing the whole history of the case, and have admirable means of for the study of pathology and morbid anatomy. This subject will never be lost sight of; for the illustration of the lectures morbid specimens are constantly brought before the notice of the pupils, or the diseases is illustrated fully as can be representation of plates on morbid anatomy … A general register of all the cases admitted into the hospital is kept, and available for statistical purposes … To enable the students to have a knowledge of vaccination, a native vaccinator attends one day in the week … and observing the true character of Jennerian Cowpock.[73]
Finally, it was concluded, the great aim is to make all the lectures and instruction as practical as possible, and to give the students that knowledge which will enable them to make their own enquiries with a case to form their own diagnosis and determine on the plan of treatment, without having their confined by nosological arrangements, or by treating a disease according to its name, rather by the general symptoms, period of disease, habits and strength of the patient.[74]
Through the banishment of “nosological arrangements” the days of the great William Cullen were gone forever, and so too the ‘humoral theory’ of disease causation.[75] Regarding “Surgical Hospital” –
With a view to establish a practical study of Surgery by the students, the formerly hired dressing men have been dispensed with, and the current duties of the Hospital are now performed by four of the senior students, who are elected “dressers” in rotation every three months – two from the European, and two from the Native pupils …
The Dressers are only allowed to perform the very minor operations of Surgery, (on the living subject) and those only by express permission of the Professor himself, in the presence of the of the students …
The four “dressers” are expected to be in attendance at the College Hospital all day, and one to reside on the premises during the, as well as the House Surgeon.[76]
Under the section “Female Hospital”, directives were clear and instructive –
In cases requiring immediate advice from the Professor in charge of the Hospital, the house surgeon shall send due notice to the former … The house surgeon shall see that the directions of the Professor in charge are obeyed.
The clinical clerks shall be selected from the senior students … They shall visit their patients at least twice daily, oftener if necessary.
In cases of labor, the clinical clerk in charge of the case must take care to be easily found when parturition begins, not absenting himself unnecessarily from home at the time when the labor is expected to come on … should not leave … until the house surgeon shall tell him that he may safely depart …
He must treat the patients kindly, with due delicacy, and take care that the nurse and other attendants give the necessary assistance and medicines when required …
It will be the duty of the house surgeon to report to the Professor the behaviour of the clinical clerks, should they misconduct themselves in any way …
The patients in the obstetric ward, shall, in lieu of diet, receive two annas per diem; their food to be cooked if they choose it by the hospital cook.[77]
It is evident from the above directives that the house surgeon was the pivot and the first responsible doctor on whom the entire process of management of the patient “kindly, with due delicacy” began and, primarily, depended too. Here a student of medicine can remember those famous warnings/sayings in the book no than Harrison’s Principles of Internal Medicine – “The hospital is an intimidating environment for most individuals. Hospitalized patients find themselves surrounded by air jets, buttons, and glaring lights; invaded by tubes and wires (in a modern hospital in the era of “techno-medicine”) … It is little wonder that a patient’s sense of reality may be compromised … they (doctors) can guide the patient through this experience may make a stressful situation more tolerable.”[78] In such a milieu, the doctor is the only tenuous link between the patient and the world of the patient. The seeds of today’s patient-centred care were contained in the 1840’s CMC teaching.
An interesting may be cited here. With the passage of time, by 1841, the gender question related to admission as a patient (not as student, to emphasize) to the CMC was almost resolved as well. The “Female Hospital” could accommodate more than one hundred patients. In 1850, the policy was worked out “to encourage women to resort to the Institution for delivery”, and, for this purpose, it became necessary to hold out many little advantages to them (‘for the present at least’) “in the shape of clothes for themselves and their children when they depart, allowances for tobacco”.[79] It certainly signifies that primarily women from lower class took resort to institutional delivery in the CMC. If they had been of the upper echelon of society, it was not necessary to provide enticements to them in the shape of clothes or tobacco. Dr. Goodeve, who was then the professor in charge of the hospital, wrote, “The number of patients has continued to increase during the past year (there are at this moment twenty women awaiting their in the Wards, and I expect others daily), in yet larger proportion than formerly, and I have no doubt, if properly managed and supported, the already established utility of this Institution will rapidly advance in importance.”[80] Providing such “advantages” might have arisen out of a threat from the indigenous practice of midwifery. Poor people were allured to institutional delivery, and this led to a gradual marginalization of indigenous practice of midwifery.
There is no doubt that almost all aspects of the clinical and hospital teachings of the students as well as the disciplined management of the hospital system were being gradually developed into its fully blossomed state step by step. And on the bedrock of such structure and management of the institution further development, progress and maturing of the institution could be materialized.
[1] William Bynum, The History of Medicine: A Very Short Description (2008), 115.
[2] Roy Porter, Blood and Guts: A Short History of Medicine (2003), 78.
[3] Porter, The Greatest Benefit to Mankind, (1999), 329.
[4] Claude Bernard, An Introduction to the Study of Experimental Medicine, tr. Henry Copley Greene (1949) 145-146.
[5] Thomas Neville Bonner, Becoming a Physician: Medical Education in Great Britain, France, Germany, and the United States, 1750-1945 (1996), 230.
[6] Ibid, 23-232.
[7] GCPI (1839), 77.
[8] Ibid, 78.
[9] GCPI (1839-40), 33.
[10] Ibid.
[11] General Report on Public Instruction, in the Bengal P4esidency for 1842-43 (hereafter GRPI), Appendix L, cii.
[12] GCPI (1839-40), 34.
[13] Ibid, 34.
[14] Ibid, 35.
[15] Ibid,35.
[16] Ibid, 36.
[17] Ibid, 36.
[18] Ibid, 36-37.
[19] Centenary, 24.
[20] GCPI (1839-40), 37-38.
[21] Ibid, 38 (footnote).
[22] David Arnold, Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth-Century India (University of California Press, 1993), 13.
[23] Arnold, “The rise of Western medicine in India”, Lancet 1996, 348 (9034): 1075-1078 (1076).
[24] Arnold, Colonizing the Body, 18.
[25] Mark Harrison, Public Health in British India: Anglo-Indian preventive medicine 1859-1914 (Cambridge University Press, 1994), 8.
[26] “Education of the Native Doctors”, Asiatic Journal 1826, 22(127): 111–21 (115).
[27] Ibid, 115.
[28] General Report of the Late General Committee on Public Instruction of 1840-41 and 1841-42, Appendix X, xciii (Hereafter GCPI, 1840-41 and 1841-42).
[29] J. Balfour, “Notes on the Branch Dispensaries Recently Opened in the Bareilly District”, Selections from the Records of the Government, North-Western Provinces, Vol. 2 (1866), 116.
[30] Ibid, 121, 125.
[31] Stephen Jacyna, “Medicine in Transformation, 1800-1849,” in The Western Medical Tradition: 1800 to 2000, W. F. Bynum, Anne Hardy, Stephen Jacyna, Christopher Lawrence, E. M. (Tilli) Tansey (2006), 11-110 (82).
[32] W. H. Sykes, “Statistics of the Government Charitable Dispensaries of India, Chiefly in the Bengal and North-Western Provinces”, Journal of the Statistical Society of London 10.1 (Mar., 1847), 1-37 (4).
[33] GCPI (1839-40), Appendix , No. VII, clxxx.
[34] Ibid, clxxx.
[35] Ibid, clxxiv.
[36] Ibid, clxxvii.
[37] Ibid, clxxix.
[38] “A Plea for Hakeems”, Indian Medical Gazette 1868, 3. (1): 87-90 (87).
[39] Ibid, 87.
[40] GRPI (1842-43), 67.
[41] David Kopf, British Orientalism: The Dynamics of Indian Modernization, 1773-1835 (1969), 184.
[42] Ibid, 183-184.
[43] GRPI (1842-43), 78.
[44] Ibid, 78.
[45] Ibid, 78.
[46] Ibid, 79.
[47] Ibid, 80-81.
[48] Ibid, 81.
[49] Ibid, 81.
[50] Ibid, 82.
[51] Ibid, 82.
[52] Ibid, 84.
[53] Ibid, 85.
[54] Ibid, 85.
[55] Ibid, 85.
[56] Ibid, 87.
[57] Ibid, 89.
[58] Rules and Regulations of the Bengal Medical College (Printed by the Order of the Council of Education, 1844 and 1849)
[59] Rules and Regulations (1844), 5.
[60] GRPI (1842-43), 90.
[61] Ibid, 90.
[62] Ibid.
[63] Ibid, 91-94.
[64] GRPI (1842-43), Appendix L, cix.
[65] Ibid, Appendix L, cxii.
[66] Rule and Regulations (1844), 32.
[67] Ranabir Ray Choudhury, ed., Calcutta: A Hundred Years Ago (Nachiketa Publications, 1988), 4. [Italics added] Note also the argument of Ulrich Trohler regarding quantification and statistics gathering – the flagship of hospital medicine. See, Trohler, Quantification in British Medicine and Surgery 1750-1830, with special reference to Its Introduction and Terapeutics, Ph.D thesis, University of London, 1978.
[68] GRPI (1842-43), Appendix L, cv.
[69] Ibid, Appendix L, cvii.
[70] Ibid, cviii.
[71] Ibid, cix.
[72] Ibid, cx.
[73] Ibid, cxi.
[74] Ibid, cxi-cxii.
[75] For a better understanding see, William Cullen, Nosology: Or a Systematic Arrangement of Diseases, by Classes, Orders, Genera, and Species; with the Distinguishing Characters of Each, and Outlines of the Systems of Sauvages, Linnaeus, Vogel, Sagar and Macbride (1800).
[76] GRPI (1842-43), Appendix L, cxiii-cxiv.
[77] Ibid, Appendix L, cxv-cxvi.
[78] Dennis L. Kasper, Anthony S. Fauci, Stephen L. Hauser, Dan L. Longo, J. Larry Jameson and Joseph Losacalzo, ed., Harrison’s Principles of Internal Medicine, 19th edition, vol. 1 (2016), 5.
[79] General Report on Public Instruction, From 1st Oct. 1849 to 30th Sept. 1850, 1851, 129. [Hereafter GRPI, 1851], 129.
[80] GRPI (1851), 129.










It’s a historic article, I can imagine how much research was done. Thanks