

(This article is a modified version of my paper under the same title published as Editorial in the Journal of Family Medicine and Primary Care 2024, 13 (5): 1589-1593)
Introductory Remarks
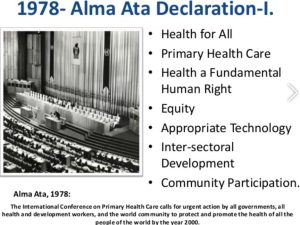
“The Alma-Ata Declaration of 1978 (6-12 September, 1978) emerged as a milestone of the twentieth century in the field of public health, and it identified comprehensive primary health care as the key to the attainment of the goal of “Health for All by 2000 A.D.”[1] It was jointly sponsored by the World Health Organization and the United Nations Children’s Fund. Some Christian Missionary groups also played a vital role in convening this international conference. “Conference on Primary Health Care (PHC) in Alma-Ata, Kazakhstan, in 1978, brought together 134 countries and 67 international organizations (China was notably absent).”[2] Chief architect of this Conference was Dr. Halfdan Mahler.[3]
The Conference emphasized on the point:
“Primary health care is essential health care based on practical, scientifically sound, and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination. It forms an integral part both of the country’s health system, of which it is the central function and main focus, and of the overall social and economic development of the community. It is the first level of contact of individuals, the family, and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first elements of a continuing health care process.”[4]
It also emphasized – “A genuine policy of independence, peace, détente, and disarmament could and should release additional resources that could well be devoted to peaceful aims and in particular to the acceleration of social and economic development of which primary health care, as an essential part, should be allotted its proper share.”[5] More specifically speaking, the Conference brought two public health related issues to the centre stage – (1) instead of disease-cantered intervention, there should be community-based programs, and (2) instead of “vertical” interventions “horizontal” interventions should be preferred in public health, and comprehensive primary health care must be prioritized.
The message of the Conference had its reverberation in the speech of Indira Gandhi too, at the 34th World Health Assembly held at Geneva, 4-22 May, 1981. Gandhi, as the prime minister of India, said:
“Life is not mere living but living in health. The health of the individual, as of nations, is of primary concern to us all. Health is not the absence of illness but a glowing vitality, a feeling of wholeness with a capacity for continuous intellectual and spiritual growth. What is our ultimate goal? Is it the mere accretion of medical and other knowledge, the building of better machines and even hospitals, or are all these meant for a higher purpose, to make man better and more capable of handling the emotional and other stresses posed by material progress, increasing pace, and the utter lack of privacy in contemporary living?”[6]
She noted in the same speech – “Dr Mahler and his colleagues deserve congratulations and encouragement on their vision of health for all by the year 2000. This envisages strengthening of public health programmes of developing countries, where most diseases are concomitants of economic backwardness.”[7]
She further added –
“We do need excellent modern hospitals. But the desire for ever larger hospitals, more often than not oriented towards high-cost modern technological medicine, has to be resisted. Primary health care must be within reach, in terms of distance as well as money, of all people … In India we should like health to go to homes instead of larger numbers gravitating towards centralized hospitals. Services must begin where people are and where problems arise … but we have not yet been able to reach out to all our rural people … Health is neither a commodity to be purchased nor a service to be given; it is a process of knowing, living, participating and being.”[8]
Transformations within the Matrix of WHO
Against this perspective, we can do some stocktaking about WHO’s gradual transformation over the years 1978 to 2024. On 21 March, 2023, WHO published a report “Commercial determinants of health”.[9] Some of the key facts enunciated were: “
“Commercial determinants of health are the private sector activities that affect people’s health, directly or indirectly, positively or negatively.
The private sector influences the social, physical and cultural environments through business actions and societal engagements; for example, supply chains, labour conditions, product design and packaging, research funding, lobbying, preference shaping and others.
Commercial determinants of health impact a wide range of risk factors, including smoking, air pollution, alcohol use, obesity and physical inactivity, and health outcomes, such as noncommunicable diseases, communicable diseases and epidemics, injuries on roads and from weapons, violence, and mental health conditions.
Commercial determinants of health affect everyone, but young people are especially at risk, and unhealthy commodities worsen pre-existing economic, social and racial inequities. Certain countries and regions, such as Small Island Developing States and low- and middle-income countries, face greater pressure from transnational actors.”[10]
Such an admittance on behalf of WHO regarding “commercial determinants of health” exposes the nature of pressure on WHO from the corporate. It also shows the helplessness of WHO as it does not have its own fund. It has to depend on various countries, organizations, and, sometimes, on some individuals. Contrarily, WHO also talks about “social determinants of health” which are “the non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life. These forces and systems include economic policies and systems, development agendas, social norms, social policies and political systems … Research shows that the social determinants can be more important than health care or lifestyle choices in influencing health.”[11] Basically, the primary issue addressed in this concept was “equity”.
In 2015, on behalf of the Third World Network, a special issue of Resurgence was published the cover of which was noteworthy – World Health Organization Corporation. David Legge commented – “The rise of the transnational corporation (TNC) as the leading agent of global governance is widely mooted. Tensions between the TNC and the nation state were on display at the recent World Health Assembly – the supreme decision-making body of the World Health Organisation (WHO) – in Geneva in May. The debates over the funding of WHO and the rules regarding WHO’s relationships with the private sector provide useful case studies for examining these apparent contradictions. The underlying forces can be mapped by exploring the links between four particular agenda items.”[12] He further elaborated – “The outcomes of these tensions will determine the prospects not just for global health but for the democratic vision and for an equitable and sustainable future.”[13] The Editorial of the same issue of Resurgence observed that “Indeed by 2013 the foundation (the Bill and Melinda Gates Foundation) was the WHO’s largest funder, providing $301 million, which exceeded United States’ combined voluntary and assessed contributions of $290 million.”[14]
David Legge commented – “The rise of the transnational corporation (TNC) as the leading agent of global governance is widely mooted. Tensions between the TNC and the nation state were on display at the recent World Health Assembly – the supreme decision-making body of the World Health Organisation (WHO) – in Geneva in May. The debates over the funding of WHO and the rules regarding WHO’s relationships with the private sector provide useful case studies for examining these apparent contradictions. The underlying forces can be mapped by exploring the links between four particular agenda items.”[12] He further elaborated – “The outcomes of these tensions will determine the prospects not just for global health but for the democratic vision and for an equitable and sustainable future.”[13] The Editorial of the same issue of Resurgence observed that “Indeed by 2013 the foundation (the Bill and Melinda Gates Foundation) was the WHO’s largest funder, providing $301 million, which exceeded United States’ combined voluntary and assessed contributions of $290 million.”[14]
Early Years of Transmutations
Within one year of the Alma-Ata Declaration, an important article was published in the esteemed medical journal New England Journal of Medicine.[15] This paper was originally presented “at a meeting on Health and Population in Developing Countries, cosponsored by the Ford Foundation, the International Development Research Center and the Rockefeller Foundation and held at the Bellagio Study and Conference Center, Lake Como, Italy, April, 1979.”[16] We must note the cosponsors of the conference. The authors of the paper argued – “Three billion people of the less developed world suffer from a plethora of infectious diseases … The best solution, of course, is comprehensive primary health care, defined at the World Health Organization’s conference held at Alna Ata in 1978”. [17] In the guise of seemingly innocuous words what they tried to do was put disease-centred programs at the centre, NOT otherwise, which they termed as “selective primary health care”.
“To emphasize, barring the period of the historical Alma-Ata Conference (1978) big corporate players of the world have always pursued the path of technology-intensive vertical care programs. Since 1960s and even before, medicine and health/healthcare have become the focus to make it a commodity of open market and private insurance. Two Nobel Laureate economists—F. A. Hayek and Kenneth Arrow—categorically advocated for such state policies. To Hayek, “there is little doubt that the growth of health insurance is a desirable development… Beveridge scheme and the whole British National Health Service has no relation to reality.”[18] Hayek did not hesitate to downplay the historical welfare health scheme NHS of the UK.
Since 1960s and even earlier, medicine and health/healthcare have become the focus of economists to make it a commodity of open market and private insurance. To Hayek, “there is little doubt that the growth of health insurance is a desirable development … Beveridge scheme and the whole British National Health Service has no relation to reality.”[19] Arrow specifically emphasized that “the subject is the medical-care industry, not health.” He even added a subtitle of one chapter as “A Survey of the Special Characteristics of the Medical-Care Market”.[20]
There appeared a few publications in quick succession – (1) Allan Enthoven prepared a draft for open/liberal market “A National-Health-Insurance Proposal Based on Regulated Competition in the Private Sector” and put it before the Carter administration. They gave him go-ahead signal. It was published in two parts in NEJM.[21] (2) In 1980, Arnold S. Relman published his historic essay.[22] (3) In 1999, an important article in Lancet showed the nexus between World Trade Organization and domestic policies of health care. The Lancet paper noted – “The WTO is stage-managing a new privatisation bonanza at Seattle. Multinational and transnational corporations, including the pharmaceutical, insurance, and service sectors, are lining up to capture the chunks of gross domestic product that governments currently spend on public services such as education and health. The long tradition of European welfare states based on solidarity through community risk-pooling and publicly accountable services is being dismantled.”[23]
In his above-mentioned paper Arnold Relman clearly showed –
“However, there has been a steady trend away from individual ownership and toward corporate control. During the past decade the total number of proprietary hospitals has been increasing again, mainly because of the rapid growth of the corporate-owned multi-institutional hospital chains … Last year, about $15 billion was spent on diagnostic laboratory services of all kinds. The number of laboratory tests performed each year in this country is huge and growing at a compound rate of about 15 per cent per year.”[24]
He also stressed – “We Americans believe in private enterprise and the profit motive. How logical, then, to extend these concepts to the health-care sector at a time when costs seem to be getting out of control, voluntary institutions are faltering, and the only other alternative appears to be more government regulation.”[25]
In later studies, researchers have identified –
“Since the 1970s, neoliberal health and social welfare policies around the world have shifted resources from the public to the private sector, reduced benefits to recipients, and affected the lives of clients and workers alike. While many researchers have studied the negative impact of these policies on the well-being of the clients of health and human service agencies, and of workers in the private sector, less is known about the adverse effect of neoliberal disinvestment on the well-being of health and human service care workers”[26].
They have emphasized that shared interests of care workers and the people they care for in the “fight-back” against neoliberalism suggest the potential for aligning care workers’ health and safety with client/patient needs in public policy formation.
Despite these consistent and powerful attempts to make community-centred health program topsy-turvy and to reduce comprehensive primary health care to “selective primary health care”, dissenting humane voices came from within the mainstream publications. Such a paper emphasized that the “trouble is that the patient, when he thinks something is wrong with him, is not an economic man. He is a fearful, ignorant, helpless, miserable creature. He does want health, almost at any price.”[27] Here we should note the term “economic man” or consumer culture in medicine. It was also clearly enunciated that the ailing and helpless person “wants no second best. He certainly does not want his needs to be weighed against the claims of other patients. The patient, in short, is looking for a trustee, not a ‘provider’.[28] Such a proposition goes starkly against – (1) equating “health” and corporate “healthcare service”, and (2) the reduction of patients to an “economic man”/consumer instead of a person.
The Intriguing Phase of Health Being “Forgotten”
Karl Evang, one of the three doctors whose efforts brought health as an agenda in international economic and political scenario, has chronicled an intriguing phase in the history of mankind. In his own words – “One interesting historic example is that health was “forgotten” when the Covenant of the League of Nations was drafted after the first World War. Only at the last moment was world health brought in, producing the Health Section of the League of Nations, one of the forerunners of the present FAO, as well as of WHO.”[29]
Further, in the same article, Evang exclaimed – “Who would have thought, therefore, that health would again be “forgotten” when the Charter of the United Nations was drafted at the end of the Second World War? However, this was exactly what happened, and the matter of world health had again to be introduced more or less ad hoc at the United Nations conference at San Francisco in the spring of 1945.”[30]
At the initiative of three doctors – Karl Evang (Norway), Paula Souza (Brazil) and. Szeming Sze (China) – health was included in the charter of UN. Evang foretold us that under circumstances where the political balance in a country was not stable rather jeopardized and where individual parties therefore had to think of something special to attract votes for the next election, this might sometimes lead to political “overbidding” in the field of health.
Concluding Remarks
Recently, Intergovernmental Negotiating Body (INB) which is tasked under WHO has drafted a new Pandemic Treaty which, it is apprehended, might be disastrous for general well-being and rightful living for citizens in future. Lancet observes that even the anaemic commitments of the agreement are in jeopardy. “Independent monitoring of whether countries are complying with their commitments is essential for the efficacy and longevity of the treaty … all indications suggest that the governance and accountability mechanisms of the treaty are being further undermined. There is little in the way of clear enforceable obligations to prevent zoonotic disease outbreaks, implement One Health principles, strengthen health systems, or counter disinformation.”[31]
To mention, one offshoot of corporatization of healthcare is “medical tourism”.
A few years ago, Raman Kumar raised three important issues which can be enumerated in the following way – (1) immediately after independence, India pushed aside the recommendations of the Bhore committee, which was for implantation of comprehensive primary healthcare. Instead, the statesmen opted for the path of selective primary care modelled on vertical disease–based programs under the guidance of international development agencies, (2) superspecialty care, fragmented public health programs, and quackery became three pillars of the Indian health system, and, finally, he asked – “Will the Indian economy be able to sustain the double burden of UHC and the vertical programs?”[32]
All these observations are very much relevant now when seen through the window of family medicine and primary care.
Bibliography/References
[1] WHO called to return to the Declaration of Alma-Ata: International conference on primary health care. World Health Organization. Available from: https://www.who.int/teams/social-determinants-of-health/declaration-of-alma-ata. [Last accessed on 2023 26 March].
[2] Primary Health Care: 25 Years of the Alma-Ata Declaration. Available from: https://www3.paho.org/english/dd/pin/alma_questions.htm. [Last accessed on 2023 8 March].
[3] Brown Theodor M. Halfdan Mahler: Architect and Defender of the World Health Organization “Health for All by 2000” Declaration of 1978. Am J Pub Health 2016; 106(1): 38-39.[4] Alma-Ata 1978: Primary Health Care (Report of the International Conference on Primary Health Care, Alma Ata, USSR, 6-12 September 1978). Geneva: World Health Organization, 1978, pp. 3-4.
[5] Alma-Ata 1978: Primary Health Care (Report of the International Conference on Primary Health Care, Alma Ata, USSR, 6-12 September 1978). Geneva: World Health Organization, 1978, pp. 5-6.
[8] Thirty-Fourth World Health Assembly, Geneva, 4-22 May, 1981. Geneva: WHO; 1981, p. 73.
[7] Thirty-Fourth World Health Assembly, Geneva, 4-22 May, 1981. Geneva: WHO; 1981, p. 73.
[8] Thirty-Fourth World Health Assembly, Geneva, 4-22 May, 1981. Geneva: WHO; 1981, p. 74.
[9] Commercial determinants of health (on the internet). WHO, 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/commercial-determinants-of-health. [Last accessed on 2023 4 April].
[10] Commercial determinants of health (on the internet). WHO, 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/commercial-determinants-of-health. [Last accessed on 2023 9 June].
[11] Social determinants of health. WHO 2024. Available from: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1. [Last accessed on 2024 29 March]
[12] Legge David. WHO shackled: Donor control of the World Health Organisation. Resurgence: World Health Organization Corporation? Resisting Coroprate Influence in WHO (Double Issue) 2015; 208-209: 15-18. Available from: https://www.twn.my/title2/resurgence/2015/298-299.htm. [Last accessed on 2024 4 April].
[13] Legge David. WHO shackled: Donor control of the World Health Organisation. Resurgence: World Health Organization Corporation? Resisting Coroprate Influence in WHO (Double Issue) 2015; 208-209: 15-18. Available from: https://www.twn.my/title2/resurgence/2015/298-299.htm. [Last accessed on 2024 4 April].
[14] Editorial. Resurgence: World Health Organization Corporation? Resisting Coroprate Influence in WHO (Double Issue) 2015; 208-209 Available from: https://www.twn.my/title2/resurgence/2015/298-299.htm. [Last accessed on 2024 4 April].
[15] Walsh Julia A. And Warren Kenneth S. Selective Primary Health Care – An Interim Strategy for Disease Control in Developing Countries. New England Journal of Medicine 1979; 301(18): 967-974.
[16] Walsh Julia A. and Warren Kenneth S. Selective Primary Health Care – An Interim Strategy for Disease Control in Developing Countries. New England Journal of Medicine 1979; 301(18): 967-974. Note at the bottom of the first page, p. 967.
[17] Walsh Julia A. and Warren Kenneth S. Selective Primary Health Care – An Interim Strategy for Disease Control in Developing Countries. New England Journal of Medicine 1979; 301(18): 967.
[18] Bhattacharya J. Comprehensive primary health care, not any vertical program needed for UHC. Journal of Family Medicine and Primary Care. 2019 Jun; 8(6):2165.
[19] Hayek FA. The Constitution of Liberty. The Definitive Edition. Chicago: University of Chicago Press; 1960: 421–422.
[20] Arrow Kenneth. Uncertainty and welfare economics of medical care. American Economic Review 1963; 53(5): 941–73. [Italics added]
[21] Enthoven Allan. Consumer-choice health plan (First of Two Parts). Inflation and inequity in health care today: alternatives for cost control and an analysis of proposals for national health insurance. New England Journal of Medicine 1978, 298(12): 650-658. Enthoven Allan. Consumer-Choice Health Plan (Second of Two Parts). A national-health-insurance proposal based on regulated competition in the private sector. New England Journal of Medicine 1978, 298(13): 709-720.
[22] Relman S. Arnold. The New Medical-Industrial Complex. New England Journal of Medicine 1980; 303(17): 963-970.
[23] Price David, Pollock Allyson M. and Shaoul Jean. How the World Trade Organization is shaping domestic policies in health care. Lancet 1999; 154(27): 1889-1892.
[24] Relman S. Arnold. The New Medical-Industrial Complex. New England Journal of Medicine 1980; 303(17): 963-964.
[25] Relman S. Arnold. The New Medical-Industrial Complex. New England Journal of Medicine 1980; 303(17): 966.
[26] Abramovitz Mimi and Zelnick Jennifer. Double Jeopardy: The Impact of Neoliberalism on Care Workers in the United States and South Africa. International Journal of Health Services 2010; 40(1): 97-117.
[27] Brewster Kingman. Health at any price? Journal of the Royal Society of medicine 1978; 72(10): 719-723.
[28] Brewster Kingman. Health at any price? Journal of the Royal Society of medicine 1978; 72(10): 720.
[29] Evang Karl. Political, National and Traditional Limitations to Health Control. In: Wolstenholme Gordon and O’Connor Maeve, editors, Health of Mankind (CIBA Foundation 100th Symposium). London: J. & A. Churchill Ltd.; 1967, pp. 196-211.
[30] Evang Karl. Political, National and Traditional Limitations to Health Control. In: Wolstenholme Gordon and O’Connor Maeve, editors, Health of Mankind (CIBA Foundation 100th Symposium). London: J. & A. Churchill Ltd.; 1967, pp. 202-203.
[31] The Pandemic Treaty: shameful and unjust. Lancet 2024; 403(10429): 781.
[32] Kumar R. Universal health coverage – Time to dismantle vertical public health programs in India. Journal of Family Medicine and Primary Care 2019; 8:1295–6.







Excellent sir.
Very nice👍👍👍 🙏🙏🙏
Emphasis on primary healthcare and community medicine had been taken a backstage since independence. I feel proud to read India’s technological advances but will be happier when healthcare (both primary and secondary) becomes an important issue in the parliamentary elections.
This requires public awareness and that is what this article brings about.
Good work Jayanta.