

(Illustration from “Cases of Organic Diseases of the Heart and Lungs,” by John C. Warren, April 1, 1812, Issue of the New England Journal of Medicine – More than 200 Years Ago)
(First issue of the Lancet -1824 – the Two Journals with the Highest Impact Factors – Lancet 168.9 & NEJM 176.082)
It is a daunting task to chart out so many ramifications of medicine spanning last 50 years within a few words or small space. However, to begin with, the emergence of “hospital medicine” from the last two decades of the 18th century to the first two decades of the 19th century (in the Paris hospitals) was the crucial watershed in the development of modern scientific medicine. It rested on three pillars – autopsy, bedside/clinical learning and accumulating medical statistics.[1] By the 1780s, the patient’s narrative was no longer the focus of inquiry in the infirmary.[2] Following Xavier Bichat’s discovery of tissues as the sites of diseases – organ localization of diseases – and the discovery of the stethoscope by Laennec in 1816, the new medicine began to shed off its old humoral legacy. Owsei Temkin, in his celebrated essay, reminds us – “Surgery, for many centuries, had relied on an objective anatomical diagnosis. In turning to a localized pathology, medicine adopted a point of view prevalent among surgeons. In part at least, the reorientation of medicine was due to an increasing approximation between medicine and surgery during the 18th century, with pathological anatomy and experimental physiology as a common ground cultivated by both disciplines.”[3] However, for brevity of space, would like to give some sketches in the development of medicine in major fields only.
Medicine
From the starting point modern medicine – hospital medicine – gradually transcended to the levels of “laboratory medicine”, “techno-medicine” and now what is being called “precision medicine”[4] – “In the decades ahead, the pace of biomedical discovery will accelerate. The state of an individual person will be characterized with increasing precision from the molecular level to the genomic level to the organ level and by interactions with medications, nutrients, the microbiome, therapeutic devices, and the environment. This precision medicine will become possible because of huge data sets on large populations, with millions of characterizations of each person. Study populations will grow to millions, which will allow observational studies with novel statistical methods that will allow discovery of useful, reproducible patterns and relationships from these data.[5]
In 1970, the first “Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter” was published. In 1981, series of reports on the outbreak community-acquired Pneumocystis carnini pneumonia (now known as HIV) were published, in 1982 – Willem Johan Kolff performs the first artificial heart transplant, in 1985 – Automated DNA sequencer – Leroy Hood and Lloyd Smith, 1985 – Polymerase chain reaction (PCR) – Kary Mullis, 1985 – Surgical robot – Yik San Kwoh, 1985 – DNA fingerprinting – Alec Jeffreys, 1985 – Capsule endoscopy – Tarun Mullick, 1986 – fuoxetine HCl – Eli Lilly and Co. in 2000 – The Human Genome Project draft was completed, in 2006 – First HPV vaccine approved, in 2011 – First successful Uterus transplant from a deceased donor in Turkey, in 2013 – The first kidney was grown in vitro in the U.S., in 2013 – The first human liver was grown from stem cells in Japan.
These are some glimpses in development of medicine in last 50 years or so. As a result, while talking about “precision medicine”, societies will come to accept that comprehensive knowledge of disease, prevention, and effective treatment is an essential public good. To remember, the medicine of the future will not, of course, solve all problems, and it cannot prevent violent or self-destructive human behaviors. Patients will continue to rely on physicians and the medical community for the guidance, support, and help that only a skilled and caring heath professional can deliver. The medical community must provide direction to ensure that powerful new technologies are used to benefit the health of all.
A few words about the development in vaccines in last 50 years should also be mentioned. After Jenner, Pasteur and Max Theiler (attenuated yellow fever virus by means of serial passage in mouse and chicken embryos in 1937), fourth breakthrough occurred in 1980, when Stanford biochemists Richard Mulligan and Paul Berg published findings from their experiments that involved transfecting monkey kidney cells with an Escherichia coli gene and thereby causing mammalian cells to make a bacterial protein. Recombinant DNA technology was born. After the introduction of Salk’s inactivated polio vaccine, for example, the incidence of polio dropped from 29,000 cases in 1955 to fewer than 900 in 1962. With the introduction of Sabin’s live attenuated vaccine in the early 1960s, polio was eliminated from the United States. Since its licensure in 2006, the bovine–human reassortant rotavirus vaccine has virtually eliminated rotavirus, preventing up to 75,000 hospitalizations and 60 deaths per year. During the 2019–2020 influenza season, the influenza vaccine prevented an estimated 7.52 million infections, 3.69 million medical visits, 105,000 hospitalizations, and 6300 deaths in the United States.
After the introduction of Salk’s inactivated polio vaccine, for example, the incidence of polio dropped from 29,000 cases in 1955 to fewer than 900 in 1962. With the introduction of Sabin’s live attenuated vaccine in the early 1960s, polio was eliminated from the United States. Since its licensure in 2006, the bovine–human reassortant rotavirus vaccine has virtually eliminated rotavirus, preventing up to 75,000 hospitalizations and 60 deaths per year. During the 2019–2020 influenza season, the influenza vaccine prevented an estimated 7.52 million infections, 3.69 million medical visits, 105,000 hospitalizations, and 6300 deaths in the United States. In addition, since the hepatitis B virus vaccine started being routinely recommended for newborns in the early 1990s, rates of hepatitis B virus infection among children younger than 10 years have fallen from about 18,000 per year to nearly zero. Now efforts are on to make vaccines is being advanced against SARS-CoV-2. New technologies are also being used. With the recent authorization of mRNA vaccines, we have entered the fifth era of vaccinology. This class of vaccines doesn’t contain viral proteins; rather, these vaccines use mRNA, DNA, or viral vectors that provide instructions to cells on how to make such proteins.[6]
In 2018, Nature published an important research paper “mRNA vaccines – a new era in vaccinology”.[7] The authors commented – “Important future directions of research will be to compare and elucidate the immune pathways activated by various mRNA vaccine platforms, to improve current approaches based on these mechanisms and to initiate new clinical trials against additional disease targets.” SARS-CoV-2 has given that possibility. Moreover, according to the paper, “Important future directions of research will be to compare and elucidate the immune pathways activated by various mRNA vaccine platforms, to improve current approaches based on these mechanisms and to initiate new clinical trials against additional disease targets.”[8]
Surgery
Before the advent of anesthesia and Listerism (asepsis) Robert Liston was acclaimed to be the fastest surgeon in the world.[9] With a humorous tone, Atul Gwande narrates his feat – “Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler’s operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant’s fingers along with a patient’s leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)”[10]
Humour apart, surgery began to progress through an increasingly important process of refinement and professionalization. Specialization was likewise an important force. But the most striking story of surgery in recent decades is how firmly it has become established as an essential tool for helping people live long and healthy lives. Virtually no one escapes having a condition for which effective treatment requires surgery — a serious orthopedic injury, a cataract, a tumor, obstructed labor, joint failure, severe cardiac disease. Today, surgeons have in their arsenal more than 2500 different procedures. Meanwhile, the practice of surgery itself will continue to change. Prognostication is a hazardous enterprise. But if the past quarter century has brought minimally invasive procedures, the next may bring the elimination of invasion. Gwande remarks – “The possibilities are tantalizing. A century into the future, a surgeon will tell the tale — that is, if the world still makes such people.”[11]
A tabulation of implantable medical devices is also important. David Schneider has comprehensively dealt with this issue.[12]
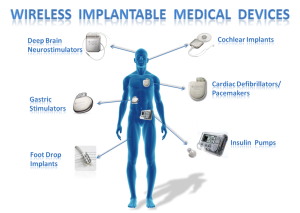
Schneider observes – “Healthcare is expensive because technological breathroughs are costly; patients who have health insurance can afford pricey solutions, and hospitals are happy to provide therapies that booster their bottom line.”[13]
What if innumerable people across the globe are without any high-priced insurances? American experience tells us a horrific story. “Shocked” wouldn’t be accurate, since we were accustomed to our uninsured patients’ receiving inadequate medical care. “Saddened” wasn’t right, either, only pecking at the edge of our response. And “disheartened” just smacked of victimhood. After hearing this story, we were neither shocked nor saddened nor disheartened.
We were simply appalled.[14] Authors remorsefully comments – “We find it terribly and tragically inhumane that Mr. Davis and tens of thousands of other citizens of this wealthy country will die this year for lack of insurance.”[15]
Midwifery
One of the most striking developments in the field of midwifery can be depicted thus – “Women at high risk for single-gene disorders or aneuploidies who want to avoid these births but find pregnancy termination unacceptable may choose preimplantation genetic diagnosis. In this process, a single blastomere is removed from each of the embryos created by means of IVF and ICSI and studied with the appropriate molecular genetic techniques to enable transfer into the uterus of only genetically normal embryos. Recognition that measurable quantities of cell-free fetal DNA appear in the maternal circulation very early in gestation has resulted in successful noninvasive prenatal diagnosis of single-gene disorders in fetuses of women known to be at risk.”[16]
But there is a cautionary note – “While those of us who provide care assume a greater stewardship role over costs and value for patients who currently have access to care, we must negotiate for adequate societal resources to bring care to those who are currently without it. As necessary and important as these achievements will be, they will seem somewhat selfish and parochial if we do not also find ways to reduce the burden of perinatal morbidity and mortality in areas of the world that presently have outcomes that are similar to those in the United States a century ago. Science and technology will undoubtedly help extend and deliver care in new ways; however, more fundamentally, progress in global obstetrical health will depend on developing the infrastructure, political will, and culture that value the health of women and their pregnancies.”[17]
Some of the Important Milestones of Cancer Reasearch
1975 Hybridomas and monoclonal antibodies – Tracking of cancer statistics by SEER program, 1976 Cellular origin of retroviral oncogenes, 1979 Epidermal growth factor and receptor, 1981 Suppression of tumor growth by p53, 1984 G proteins and cell signalling, 1986 Retinoblastoma gene, 1990 First decrease in cancer incidence and mortality, 1991 Association between mutation in APC gene and colorectal cancer, 1994 Genetic cancer syndromes Association between BRCA1 and breast cancer, 2000 Sequencing of the human genome, 2002 Epigenetics in cancer MicroRNAs in cancer, 2005 First decrease in total number of deaths from cancer, 2006 Tumor stromal interaction, 2015 Talimogene Laherparepvec, 2017 CAR T-Cell Therapies, 2017 Genomic Profiling Tests, 2018 NCI-Sponsored TAILORx Clinical Trial, 2020 International Pan-Cancer Analysis of Whole Genomes.
Important aspects remaining outside the gamut of this article are – (1) Evolving Roles of the Medical Journal, (2) History of Health Law, (3) Development in Hospital Costs and Mortality, (4) Developments in Diabetic Care, and (5) Health as Human Right.
Regarding patient-doctor relationship the crux of the question has been has been aptly summarized as – “Clinical research is no longer regarded as a side benefit of providing patients with clinical care, but rather as a compatible but distinct activity that requires us to view patients as partners in the process of advancing medical knowledge. And finally, the greatest challenge still lies largely before us, as we will struggle in the years to come to balance the personal advocacy that all patients rightfully expect from their physicians with the equally compelling obligation of physicians to see that health care resources are used wisely in ways that are efficient and fair.”[18]
Concluding Remarks
The right to health is a fundamental part of our human rights and of our understanding of a life in dignity. The right to the enjoyment of the highest attainable standard of physical and mental health, to give it its full name, is not new. Internationally, it was first articulated in the 1946 Constitution of the World Health Organization (WHO), whose preamble defines health
as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. The preamble further states that “the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.” The 1948 Universal Declaration of Human Rights also mentioned health as part of the right to an adequate standard of living (art. 25). The right to health was again recognized as a human right in the 1966 International Covenant on Economic, Social and Cultural Rights.
Declaration of Alma-Ata, 1978 – Which Constitutes a Distinct Watershed in the Area of Health and Human Right
The Declaration affirms the crucial role of primary health care, which addresses the main health problems in the community, providing promotive, preventive, curative and rehabilitative services accordingly (art. VII). It stresses that access to primary health care is the key to attaining a level of health that will permit all individuals to lead a socially and economically productive life (art. V) and to contributing to the realization of the highest attainable standard of health.
The right to health is also recognized in several regional instruments, such as the African Charter on Human and Peoples’ Rights (1981), the Additional Protocol to the American Convention on Human Rights in the Area of Economic, Social and Cultural Rights, known as the Protocol of San Salvador (1988), and the European Social Charter (1961, revised in 1996).
The American Convention on Human Rights (1969) and the European Convention for the Promotion of Human Rights and Fundamental Freedoms (1950) contain provisions related to health, such as the right to life, the prohibition on torture and other cruel, inhuman and degrading treatment, and the right to family and private life. Finally, the right to health or the right to health care is recognized in at least 115 constitutions. At least six other constitutions set out duties in relation to health, such as the duty on the State to develop health services or to allocate a specific budget to them.[19]
________________________________________
[1] For very good insightful analyses see, Erwin Ackerknecht, Medicine at the Paris Hospital, and Roy Porter, The Greatest Benefit to the Mankind, and Joam Lane, Social History of Medicine.
[2] Marry E. Fissel, “The disappearance of the patient’s narrative and the invention of hospital medicine,” in British Medicine in an Age of Reform, eds., Roger French and Andrew Wear (London, New York: Routledge, 1991), 92-109 (99).
[3] Owsei Temkin, “The Role of Surgery in the Rise of Modern Medical Thought”, Bull Hist Med, 1951, 25 (3): 248-259.
[4] Isaac Kohane, Jeffrey Crazen and Edward Campton, “A Glimpse of the Next 100 Years of Medicine”, NEJM 2012, 376 (26): 2538-2539.
[5] Ibid, 2558.
[6] Angella Desmond and Paul Offit, “, “On the Shoulders of Giants – From Jenner’s Cowpox to mRNA Covid Vaccines”, NEJM 2021, 384 (12): 1081-1083.
[7] Norbert Pardi, Michael Hogan, Frederick Porter and Drew Weissman, “mRNA vaccines – a new era in vaccinology”, Nature, 2018 (17): 261-279.
[8] Ibid, 276.
[9] Kaushik Bhattacharya & Neela Bhattacharya, “Robert Liston – “The Surgeon with the Fastest Knife”, Indian Journal of Surgery, 2022 (84): 1311-1314.
[10] Atul Gwande, “Two Hundred Years of Surgery”, NEJM 2012, 366 (18): 1716-1723.
[11] Ibid, 1722.
[12] David Schneider, The Invention of Surgery – A History of Modern Medicine: From the Renaissance to the Implant Revolution (London: Coronet, 2020).
[13] Ibid, 327.
[14] Michael Stillman and Monalisa Tailor, “Dead Man Walking”, NEJM 2013, 369 (20): 1880-1881.
[15] Ibid, 1881.
[16] Michael Green, “Two Hundred Years of Progress in the Practice of Midwifery”, NEJM 2012, 367 (18): 1732-1740.
[17] Ibid, 1739.
[18] Robert D. Truog, “Patients and Doctors – The Evolution of a Relationship”, NEJM 2012, 366 (7): 581-585.
[19] WHO, “The Right to Health”, Fact Sheet No. 31.










I should thank you for writing such rich articles regularly and maintaining a careful approach in explaining the issues in such sweet choice of words that and a reader with average knowledge like me may also understand the basic views.
Primary health is said to have been approved to be basic concern for all countries for raising health standards of their people. They made promises. But promises are made not for continuous attention and priorities change with time and political power.
International health system is now controlled by international pharmaceutical companies and by constitutional powers.