

চতুর্থ অধ্যায় – নার্সিংয়ের সূচনা
১৫ জুন, ১৮৬৪, মেডিক্যাল কলেজের প্রিন্সিপাল Norman Chevers “ইন্ট্রোডাক্টরি লেকচার” দিলেন ছাত্রদের সামনে। লেকচারের শিরোনাম “The Physician’s Calling”। লেকচারের শেষাংশে বললেন – “একজন শুভ্রকেশ বৃদ্ধের চোখ চকচক করে উঠবে যখন তোমাদের প্রথম হবার পুরষ্কার তাঁকে দেখাবে, কিংবা যখন বলবে তাঁর ছেলে ডক্টর অফ মেডিসিন (এমডি) হয়েছে, যখন কোন মুমূর্ষু রোগী পরম কৃতজ্ঞতায় তোমার হাত চেপে ধরবে, যখন তোমার স্মৃতিতে আসবে কোন কুলি বা মুটের স্ত্রীর শয্যার পাশে রাত জেগেছ তার “difficult labor”কে সফল করার জন্য, কিংবা কোন বৃদ্ধার দান করা সোনা তুমি প্রত্যাখ্যান করেছ কারণ ওই সোনা তোমার চেয়ে তার মাতৃহারা সন্তানদের বেশি প্রয়োজন … কখনও ভুলবেনা যে সবচেয়ে সফল চিকিৎসক সে যে এই জীবনের ওপারে “has best assurance of approval in the Life to Come.” (“The Physician’s Calling”, পৃঃ ১২)
প্রায় হুবহু একই কথা, ভিন্ন ঢংয়ে, বলেছিলেন J. Warburton Begbie তাঁর “Course of Clinical Instruction” শীর্ষক “ইন্ট্রোডাক্টরি লেকচার”-এ “ordinary physicians of the Royal Infirmary, Edinburgh”-এর সামনে একই বছরে ৭ নভেম্বর, ১৮৬২ সালে (ল্যান্সেট, ২২ নভেম্বর, ১৮৬২, পৃঃ ৫৫৫)। Begbie তাঁর লেকচারে বললেন – “should we not constantly act as if our experience might, on any day or hour, be that of the poet?
Tread softly! bow the head —
In reverent silence bow!
No passing bell doth toll;
Yet an immortal soul Is passing now.” (প্রখ্যাত ইংরেজ কবি রবার্ট সাদির স্ত্রী ক্যারোলাইন বোলস সাদি ১৮৬৬ সালে “Pauper’s Death-Bed” নামে এই কবিতাটি লিখেছিলেন। সে কবিতার প্রথম ছত্র।)
Chevers তাঁর “ইন্ট্রোডাক্টরি লেকচার”-এর শুরুতে অসীম মহিমাময় ঈশ্বর সম্বন্ধে অনেকটা জায়গা ব্যয় করেছেন। তাঁর অভিমতে যাদের চৈতন্য নিষ্প্রভ তারা কখনও ভালো চিকিৎসক হতে পারেনা। নিজের বিশ্বাসের প্রতিই সে বিশ্বস্ত থাকতে পারেনা। (“The Physician’s Calling”, পৃঃ ৩) বললেন – “এই মহৎ বিজ্ঞান দুটি বৃহৎ ধারায় বিভক্ত – Prevention and Remedy” এবং স্যানিটেশন”। (পৃঃ ৪) এরপরে কতকগুলো বিশেষ বিষয়ের উত্থাপন করলেন যা পূর্ববর্তী বার্ষিক রিপোর্টগুলোতে বলা হয়নি – “শরীরের অঙ্গসংস্থান বোঝার জন্য অ্যানাটমি, “he then acquires the knowledge of the vital actions or functions of animal bodies, which is called Physiology … these vital actions as perverted and modified in disease … Pathology”। যে ফিজিওলজি এবং প্যাথলজি সম্পর্কে অজ্ঞ সে আসলে অপরাধ করছে”। (পৃঃ ৬) স্যানিটেশন নিয়ে কেন ১৮৬৪ সালের ভাষণে গুরুত্ব দিলেন তার কারণ আমরা একটু পরে বুঝতে পারব। তার আগে তাঁর লেকচারটি নিয়ে সামান্য কিছু কথা বলে নিই। তিনি জোর দিলেন থিওরেটিক্যাল জ্ঞানের চেয়ে হাসপাতাল ওয়ার্ডে রোগী দেখা এবং শিক্ষকদের নোটের ওপরে – “As students, you will do well to imitate the example of Descartes, having a small library, and learning more from men and experiments than from books.” (পৃঃ ৮) Scientific periodicals পড়ার ওপরেও জোর দিলেন। (পৃঃ ৯) বললেন – চিকিৎসকদের পরিবারের কোন সদস্যের কাছ থেকে পেশাগত ফি নেওয়া যাবেনা, এবং “ought not to receive a fee from a Minister of Religion”। (পৃঃ ১১)
Chevers-এর বক্তৃতার সাথে আমরা যদি উইলিয়াম টি গার্ডিনার-এর Royal Infirmary of Edinburgh-তে দেওয়া বক্তৃতার (“A Lecture on the Study of Clinical Medicine”, ল্যান্সেট, জানুয়ারি ২৫, ১৮৬২, পৃঃ ৯৩-৯৫) প্রতিতুলনা করি তাহলে জ্ঞানের “কেন্দ্র” তথা মেট্রোপলিটান এবং জ্ঞানের উপনিবেশিক “প্রান্ত”-এর শিক্ষাদানের পদ্ধতির পার্থক্য সহজেই বোঝা যাবে। গার্ডিনার প্রধানত হাসপাতাল ওয়ার্ডে শিক্ষাদানের বিষয়ে নির্দিষ্ট আপত্তি জানিয়ে বলেছিলেন “thinking aloud” শিখতে হবে ছাত্রদের। বিভিন্ন বিষয়ে নিজেদের যুক্তির অবতারণা করে ছাত্রদের তর্ক করতে শিখতে হবে। শিখতে হবে নিজের হাতে ল্যাবরেটরিতে প্রস্রাব এবং অন্যান্য প্রয়োজনীয় পরীক্ষা করা। ছাত্রদেরকে Outline Figures for recording Physical Diagnosis, for the use of Students and Practitioners of Medicine (Edinburgh, 1862) থেকে “to obtain these diagrams, and to employ them habitually in the wards” ব্যবহার করার কাজটি আয়ত্ত্ব করা শিখতে হবে।
প্রাক- Chevers আন্তর্জাতিক মেডিসিনের জগতের অতি-সংক্ষিপ্ত চালচিত্র
আর্তুরো কাস্তিগ্লিওনি (Arturo Castiglioni) তাঁর সুবিশাল পুস্তক A History of Medicine (tr. E. B. Krumbhaar, ১৯৪৭)-এ ভির্শোর সেলুলার প্যাথলজি এবং এর অভিঘাতে মেডিসিনের অন্তর্বস্তু বদলে যাওয়া নিয়ে মন্তব্য করেছেন – “The cell doctrine,” he (ভির্শো) wrote, “applied to all living structures, leads to a cellular physiology and a cellular pathology, which is always based on histology — that is, on the anatomic knowledge of the structural elements.” Virchow’s book outlined a new and important orientation for scientific medicine, although, of course, he was not able to solve all the problems of pathology or always to arrive at accurate generalizations.”
ফিজিওলজির নতুন বোধ মেডিসিনের জন্য কি পরিবর্তন আনল বোঝাতে গিয়ে বলছেন- “১৮৫৭ সালের মধ্যে লিভারের যে গ্লুকোজ তৈরির ক্ষমতা রয়েছে এই ধারণা যথেষ্ট প্রতিষ্ঠিত হয়ে গিয়েছিল; গ্লাইকজেনকে পৃথক করা সম্ভব হয়েছিল এবং জানা ছিল মাংসপেশির কাজের জন্য গ্লাইকোজেনের প্রয়োজন। এ সমস্ত পরীক্ষা-নিরীক্ষাগুলো যা থেকে ডায়াবেটিসের ক্ষেত্রে গ্লাইকোজেনের ভূমিকা বোঝা যাচ্ছিল ক্লদ বার্নার্ডকে এন্ডোক্রিনোলজির একজন গুরুত্বপূর্ণ পথিকৃৎ হিসেবে প্রতিষ্ঠিত করল।” (প্রাগুক্ত, পৃঃ ৬৮৩)
কেমিস্ট্রি ছাড়াও ফিজিক্সও প্রবেশ করতে শুরু করল ফিজিওলজিতে – মানবশরীরের আভ্যন্তরীন এবং বাহ্যিক গতিময়তা ও এর অন্তর্নিহিত ব্যাখ্যা বোঝার ক্ষেত্রে। এক্ষেত্রে প্রথম যে নামটি আমাদের স্মরণ করতে হবে তিনি হলেন লুডভিগ ফন হেলমহোলৎজ (Ludwig von Helmholtz)। আর্তুরোর পর্যবেক্ষণে – “Most important of all of his (Helmholtz) contributions to general science was his monograph Uber die Erhaltung der Kraft (1847), which gave the general application of the law of the conservation of energy … This established the first law of thermodynamics: that all kinds of energy can be transformed from one form to another but cannot be destroyed or created … In acoustics, he announced the doctrines of tonal sensations as a physiological basis of the theory of music.” (প্রাগুক্ত, পৃঃ ৬৮৮-৬৮৯)
নতুন মেডিসিনের চরিত্র নিয়ে ভির্শোর নিজের অভিমত ছিল – “in my opinion – the most essential point – that, whether we compare large or small, pathological or physiological cells, we always find this correspondence between them.” (Cellular Pathology, 1860, পৃঃ ২৩)
এবার বোঝা যাবে কেন ১৮৬৪-তে Chevers ফিজিওলজি এবং প্যাথলজি শেখার ওপরে গুরুত্ব আরোপ করছেন। কেন স্যানিটেশনের প্রসঙ্গই বা এল তাঁর বক্তৃতায় এর কারণও নিহিত আছে খোদ ইংল্যান্ডের মিলিটারি প্রয়োজনের মাঝে। সরকারি রিপোর্ট থেকে জানা যায় – “The high mortalities among British and Indian troops and in the civil population attracted the attention of Parliament and in 1860 a Royal Commission visited India and made recommendations for the improvement of health and sanitary condition in India.” (“Annual Report of the All-India Institute of Hygiene and Public Health for the Year 1934”, Indian Medical Gazette, Sept., 1935, পৃঃ ৫৩৩-৫৩৭)
১৮৬২ সালে খ্যাতনামা চিকিৎসক এবং প্রভাবশালী ইংরেজ কর্তাব্যক্তি W. J. Moore-এর লেখা প্রকাশিত হয়েছিল ল্যান্সেট-এ “Remarks on Indian Hill Stations: With Especial Reference to Their Sanitary Condition” (Lancet, Sept. 6, 1862, পৃঃ ২৫২-২৫৪) শিরোনামে। এ প্রবন্ধে মূর বললেন – “১৮৪৫ সালে বোম্বেতে অতিরিক্ত মৃত্যুহারের জন্য – মৃত্যুহার কোনসময়েই প্রতি ১০০০-এ প্রতিবছরে ১০১ জনের কম ছিলনা এবং ১৮৪২ সালে সেটা বেড়ে ২০৩.৭ জন প্রতি ১০০০-এ হয় – বোম্বে থেকে সৈন্যদের পুণা এবং কুকীতে স্থানান্তরিত করা হয়। ১৮৫৫ এবং ১৮৫৬ সালে মৃত্যুহার কমে প্রতি ১০০০-এ ৯ জনে এসে দাঁড়ায় ‘who would otherwise have been subjected to the mortality hitherto inseparable from a soldier’s life in Bombay’.” (Lancet, পৃঃ ২৫২) তিনি আরও বলেন যে “The history of Mahamaree, or Indian plague” যা গোড়ার দিকে হিমালয় অঞ্চলকে তছনছ করেছিল “affords an example of what will arise from defective sanitation and hygiene … and also a striking instance of the success of preventive measures in arresting the progress of epidemic disease.” (Lancet, September 13, 1862, পৃঃ ২৮১)
১৮৬২ সালেই প্রকাশিত তাঁর লেখা Health in the Tropics; or, Sanitary Art Applied to Europeans in India বইতে কর্নেল হজসনকে উদ্ধৃত করে মূর জানাচ্ছেন – “the British soldier who now serves in Bengal one year encounters as much risk of life as in three such battles as Waterloo.” (পৃঃ ১৩) ওয়াটারলুর মতো তিনটি রক্তক্ষয়ী যুদ্ধে সৈনিকদের প্রাণহানির যে আশঙ্কা থাকে বাংলায় একবছর চাকরি করলে প্রাণহানির সেরকম ঝুঁকি থেকে যায়। মূর জানাচ্ছেন সেসময়ে ভারতে মোটের ওপরে ৮০,০০০ ব্রিটিশ সৈন্য ছিল। (পৃঃ ৩) সাম্প্রতিক গবেষণায় জানা যাচ্ছে – “শত শত সৈন্যকে হারানো, যাদের প্রত্যেকের প্রশিক্ষণের জন্য রাষ্ট্রের খরচ হয়েছে £100, এর পেছনের কারণ হচ্ছে স্যানিটারি নিয়মকানুনকে উপেক্ষা করা, এবং, একথাও যোগ করা যায় যে মেডিক্যাল বিভাগের দীর্ঘকালীন অবক্ষয়।” (Michelle Allen-Emerson, Tina Young Choi, Christopher S Hamlin, ed., Sanitary Reform in Victorian Britain, Part I, Vol. I, পৃঃ ২৪৭) মূর তাঁর পূর্বোক্ত গ্রন্থে জানিয়েছিলেন – “All these facts are now matters of public notoriety, and, in future, it may well be demanded, why any military body suffers from a large percentage of disease … especially zymotic diseases, is preventable or at least mitigable.” (মূর, প্রাগুক্ত, পৃঃ ৬)
ব্রিটিশ সরকার এ পরিস্থিতি খতিয়ে দেখার জন্য “Sanitary Commission for Bengal, 1864-65” গঠন করে। কমিশনের প্রথম বার্ষিকী রিপোর্টে বলা হয় – “A Chair of Hygiene was established during the past year in connection with the Calcutta Medical College, and the Secretary to the Sanitary Commission was appointed to be the first Professor. Lectures on many subjects affecting the public health were delivered during the last season.” (First Annual Report of the Sanitary Commission for Bengal, 1864-65, পৃঃ ৬৫) মেডিক্যাল কলেজের পাঠ্যক্রমের মধ্যে রাষ্ট্রের উদ্যোগে জনস্বাস্থ্য আলাদা বিষয় হিসেবে অন্তর্ভুক্ত হল প্রথমবারের জন্য।
মার্ক হ্যারিসনের অভিমত অনুযায়ী – সিপাহী বিদ্রোহের পরে, ১৮৫৯ সালে, “a special commission was set up to inquire into the sanitary state of the British Arny in India … there was increasing concern over military hygiene in India.” ১৮৬৩ সালে এই কমিশনের রিপোর্ট ব্রিটেনে শোরগোল ফেলে দেয় এবং স্যানিটারি সংস্কার করার উপযুক্ত পরিবেশ তৈরি করে। পরিণতিতে “resulted in the establishment of sanitary commissions to monitor conditions in and around military cantonments.” (Mark Harrison, Public Health in British India: Anglo-Indian Preventive Medicine, 1859-1914, পৃঃ ৮) একথাগুলো ওপরে আলোচিত হয়েছে। গুরুত্বপূর্ণ হচ্ছে “conditions in and around military cantonments” অংশটি। ক্যান্টনমেন্টের চারপাশ পরিচ্ছন্ন রাখতে হবে – এর অনুসারী হল ক্যান্টনমেন্টকে ঘিরে থাকা ভারতীয় জনজীবনের ক্ষেত্রেও স্যানিটারি সংস্কার করতে হবে। অর্থাৎ, স্বাভাবিক উপসিদ্ধান্ত অনুযায়ী, পাবলিক হেলথ আবশ্যিক বিষয় হবে ডাক্তারি পাঠ্যক্রমে।
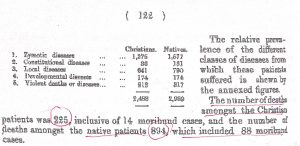
নীচের টেবিল দুটি থেকে ইউরোপীয় এবং দেশীয় সৈন্যদের মৃত্যুহারের একটি তুলনামূলক চিত্র পাওয়া যাবে।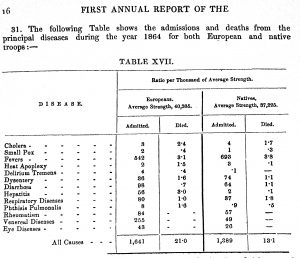
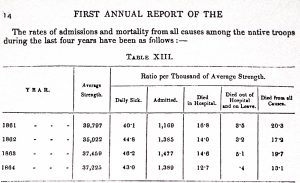
(First Annual Report of the Sanitary Commission for Bengal, 1864-65, পৃঃ ১৬, ১৪)
প্রসঙ্গত বলা দরকার, ১৮৬১ সালে “Chair of Dentistry” তৈরি করা হয়। ১৮৬৪ সালে সরকারের তরফে একটি কমিটি তৈরি করা হয় “for the purpose of enquiring into the number of Medical officers requisite for Calcutta, as it was thought “undesirable to maintain a large number of officers in Calcutta whose time was mainly occupied in private practice.” (Centenary of the Medical College, 1835, পৃঃ ৪৫)
এ বক্তব্যের সমর্থন মিলবে সরকারি রিপোর্টে, যে রিপোর্টের কথা ওপরে উল্লেখ করেছি। নীচে দেখুন।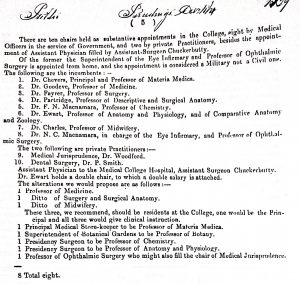
(Proceedings of The Government of India, Home Department – Public, 1864, পৃঃ ১৩৩৯)
যাহোক, ইংল্যান্ডে এবং ইউরোপের দেশগুলোতে শিক্ষাজগতের মৌলিক রূপান্তর দেরীতে হলেও গৃহীত হল মেডিক্যাল কলেজের শিক্ষাক্রমে। “A Resident and Professor of Physiology and a Resident and Professor of Pathology were also sanctioned.” এই পরিবর্তনগুলো হল ১৮৭১ সালে। (Centenary, পৃঃ ৪৫) “The same Committee took into consideration another important subject, namely, the status, training, pay and pension of the subordinate medical service – Indian and European. The recommendations submitted were embodied in a General Order (No. 550 of 5th June, 1868), which improved the position of both services very materially.” (Centenary, পৃঃ ৪৫)
১৮৬৩-৬৪ সালের শিক্ষাবর্ষের রিপোর্ট
এই রিপোর্ট বিস্তৃতভাবে জানানোর আগে উপরে উল্লেখিত সরকারি রিপোর্টের একটি পর্যবেক্ষণ উল্লেখ করা প্রয়োজনীয়। রিপোর্টে বলা হল – “এটা সত্যি যে কলকাতা মেডিক্যাল কলেজ ইউরোপীয় মেডিক্যাল স্কুলগুলো থেকে পৃথক এই অর্থে যে কলকাতা মেডিক্যাল কলেজে ৩ শ্রেণীর ছাত্র আছে (প্রাইমারি ক্লাস, মিলিটারি ক্লাস এবং বেঙ্গলি ক্লাস) যেখানে ইউরোপীয় মেডিক্যাল স্কুলগুলোতে কেবলমাত্র ১ শ্রেণীর ছাত্রদের শিক্ষা দেওয়া হয়। এখানে ইংলিশ ক্লাসই একমাত্র ক্লাস যার জন্য সর্বক্ষণের ইউরোপীয় প্রোফেসরদের প্রয়োজন পড়ে, কিন্তু এছাড়াও, হিন্দুস্তানি এবং মিলিটারি ক্লাস রয়েছে … মিলিটারি ক্লাসের ছাত্ররা বাধ্যতামূলকভাবে সিপাহী হিসেবে গণ্য হয় এবং সেনাবাহিনীতে নেটিভ ডক্টর হিসেবে যোগ দেয়, যেখানে বেঙ্গলি ক্লাস থেকে পাস করা ছাত্ররা সরকারি চাকরিতে যোগ দিতেও পারে নাও পারে।” (Proceedings of The Government of India, Home Department – Public, 1864, পৃঃ ১৩৩৮)
১৮৬৩-৬৪ সালের রিপোর্টের গোড়ার দিকেই জানানো হল, “মেডিক্যাল শিক্ষা সাধারণভাবে ব্যয়বহুল এবং রাষ্ট্রের ওপরে এ খরচ বহনের যে চাপ সেটা বাস্তবত ভবিষ্যতে কমার সম্ভাবনা নেই। মেডিক্যাল কলেজের একজন আন্ডারগ্র্যাজুয়েট ছাত্রের জন্য খরচ হয় বার্ষিক ৫৩২ টাকা, এবং এই খরচের ৫০৩ টাকা বা ৯৪% আসে সরকারের কাছ থেকে।” (GRPI 1863-64, পৃঃ ৪৫) বেঙ্গলি ক্লাসের ক্ষেত্রে পূর্ববর্তী শিক্ষাবর্ষ থেকে ৫ টাকা মাসিক মাইনে ধার্য করা হয়েছিল এবং “it is gratifying to find that no less than 32 candidates enrolled themselves as paying students.” (GRPI 1863-64, পৃঃ ৪৭) মার্ক হ্যারিসন খুব স্পষ্ট ভাষায় বলেছেন – “The emergence of what contemporaries celebrated as ‘rational’ or ‘scientific’ medicine (আগের অধ্যায়ে ইটওয়েলের ভাষণ দ্রষ্টব্য) was therefore intimately bound up with Britain’s commercial and imperial interests”। (Mark Harrison, Medicine in An Age of Commerce and Empire, 2010, পৃঃ ২৯১)
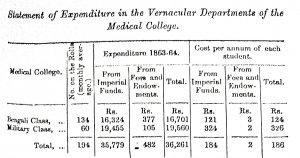
(GRPI 1863-64, পৃঃ ৪৭)
Norman Chevers প্রিন্সিপালের রিপোর্টে খোলাখুলি বললেন – “Long and observant experience of education in this part of India has convinced me that many otherwise judicious teachers labour under an impression that a certain amount of laxity of discipline, such as would never be permitted to enter into the system of any European School or College, is unavoidable in educating Bengali youths.” (GRPI 1863-64, Appendix A, পৃঃ ৪১৩) সহজ কথায় বললে, অনেক ইংরেজ বিচক্ষণ শিক্ষকও বাঙ্গালী ছাত্রদের মাঝে শৃঙ্খলার ক্ষেত্রে যে শিথিলতা ও অমনোযোগিতা আছে, যা কখনই ইউরোপীয় মেডিক্যাল স্কুল বা কলেজে বরদাস্ত করা হবেনা, তাকে এড়ানো সম্ভব নয় বলে মনে করেন। ফলে এদেরকে স্বাভাবিক পারিবারিক ও সামাজিক পরিবেশের বাইরে নিয়ে এসে ইউরোপীয় ধরণের কঠোর শৃঙ্খলায় প্রশিক্ষিত করতে হবে। (GRPI 1863-64, Appendix A, পৃঃ ৪১৪) প্রসঙ্গত, জয়ন্ত ভট্টাচার্যের মেডিক্যাল কলেজের ইতিহাস (১৮২২-৬০) পুস্তকে মেডিক্যাল কলেজের প্রথম প্রিন্সিপ্যাল ব্রামলে মেডিক্যাল কলেজের জন্মলগ্নে (১৮৩৫-৩৬ সালে) ছাত্রদের ক্ষেত্রে কিভাবে এ সমস্যার সম্মুখীন হয়েছিলেন ও সমাধান করেছিলেন তার বিস্তৃত বিবরণ রয়েছে। এখানে সে ঘটনারই পুনরাবৃত্তি দেখছি।
এখানে বিবেচনার যোগ্য আরেকটি বিষয়ও আছে। Chevers-এর বক্তব্যের মাঝে অনুক্ত এবং অন্তর্লীন হয়ে আছে racial superiority-র ধারণা। অন্যান্য বিষয়ে তো বটেই, পারিবারিক পরিবেশ, সন্তানদের মানুষ করা, ছাত্র হিসেবে গড়ে ওঠা এবং ইউরোপীয় শিক্ষার সাথে খাপ খাইয়ে নেবার ক্ষেত্রের মত বিষয়েও ইংরেজ তথা ইউরোপীয়রা যে ভারতের তুলনায় সভ্যতার মানদণ্ডে ওপরের ধাপে রয়েছে – রিপোর্টের পর্যবেক্ষণে একথাগুলো পরিষ্কার করেই বোঝানো হয়েছে। ঐতিহাসিক ওয়ারউইক অ্যান্ডারসনের মন্তব্য এক্ষেত্রে ভেবে দেখার মতো। ফিলিপিন্সে আমেরিকার ফিলিপিনোদের সুসভ্য করে তোলার জন্য “public health citizenship”-এর ধারণায় সিঞ্চিত করার পরিপ্রেক্ষিতে তিনি বলছেন – “A complex circulation and repatterning of practices of public health emerged, flexibly coupled with ideas of race and development, and as these models passed from place to place they would be readjusted before moving on.” (Warwick Anderson, Colonial Pathologies: American Tropical Medicine, Race, and Hygiene in the Philippines, 2006, পৃঃ ২৩৩) একথা সমানভাবে প্রযোজ্য ভারত, চীন বা অন্য কোন দেশের ক্ষেত্রেও।
Chevers তাঁর রিপোর্টে জানালেন যে বিগত শিক্ষাবর্ষে এমডি পরীক্ষায় মেডিক্যাল কলেজের একজন ছাত্রও পাস করেনি। ১১ মার্চ, ১৮৬৪, তারিখে গত বছরের উজ্জ্বল ২ জন এমডি পাস করা ছাত্রকে – মহেন্দ্রলাল সরকার এবং জগবন্ধু বোস – ইউনিভার্সিটি কনভোকেশনে জনসমক্ষে ডিগ্রি দেওয়া হয়। (GRPI 1863-64, Appendix A, পৃঃ ৪১৪)
এই শিক্ষাবর্ষে সিংহল থেকে কোন নতুন ছাত্র আসেনি। Chevers মনে করেছিলেন – “Considering that the students of the primary class and especially those Ceylon students who are resident within the walls of the College” তাদের মানসিক বিনোদনের জন্য চিকিৎসার জগতের বাইরের পত্রিকা রাখা দরকার। এই লক্ষ্যে “Blackwood’s and Frazer’s Magazines, the Saturday Review, and the Overland News” ইত্যাদি ম্যাগাজিন ৬ সেট করে পরীক্ষামূলকভাবে লাইব্রেরিতে রাখা শুরু হয়। (প্রাগুক্ত, পৃঃ ৪১৫) এখানে বলা দরকার যে ভারতবর্ষের ক্ষেত্রে মেডিক্যাল কলেজেই প্রথম আবাসিক শিক্ষা চালু করা হয়। পরবর্তীতে ভারতবর্ষের অন্যান্য শিক্ষা প্রতিষ্ঠানে এ পদ্ধতি অনুসৃত হয়েছে। (জয়ন্ত ভট্টাচার্য, মেডিক্যাল কলেজের ইতিহাস (১৮২২-১৮৬০) , ২০২২, দ্রষ্টব্য)
এই শিক্ষাবর্ষের একটি উল্লেখযোগ্য বিষয় হল “Students’ Society was formed”। অনেকটা বর্তমান ছাত্র ইউনিয়নের আদিরূপ বলা যেতে পারে। তবে সরকারের নিজের তৈরি, ছাত্রদের তৈরি করা নয়। স্টুডেন্টস সোসাইটির মাসিক মিটিংয়ে “essays on important subjects in medical and surgical science are read and freely discussed by the pupils.” এই মিটিংয়ে শিক্ষকদেরও আমন্ত্রণ জানানো হত। শিক্ষকেরা “have expressed surprise and pleasure at the knowledge and great readiness displayed by many of the debates.” (প্রাগুক্ত, পৃঃ ৪১৬) মনে রাখা দরকার, এসমস্ত কার্যকলাপ সীমাবদ্ধ ছিল কেবলমাত্র প্রাইমারি তথা ইংলিশ ক্লাসের ছাত্রদের জন্য।
মিলিটারি ক্লাসের ছাত্রদের ব্যাপারে রিপোর্টে বলা হয় যে যেহেতু কলেজের বাইরে রাত কাটালে “small nightly fine” দিতে হত, এ কারণে ছাত্ররা এই ফাইন দিয়েও লাগামছাড়া ভাবে বাজারে যেত এবং “often acquired the vice and dissipation (উচ্ছৃঙ্খলতা অর্থে) which impaired their health and unfitted them to become useful medical servants”। একে কড়া হাতে দমন করা হয়। (প্রাগুক্ত, পৃঃ ৪১৭)
বেঙ্গলি ক্লাসের ব্যাপারে বলা হয় যে “so many were willing to pay a very small monthly sum of their education in this class must be regarded as a very encouraging circumstance”। এ বছরেই প্রথবারের জন্য বেঙ্গলি ক্লাসে “paying class”-এর প্রবর্তন করা হয় পরীক্ষামূলকভাবে। (প্রাগুক্ত, পৃঃ ৪১৭) এরপরে লাইব্রেরি, মিউজিয়াম, ডিসেকটিং রুম এবং হাসপাতালের যথানিয়মে বিবরণ দেওয়া হয়েছে।
এই শিক্ষাবর্ষের অধিকতর গুরুত্বপূর্ণ বিষয় হল “Bachelor of Medicine” বা এমবি পরীক্ষার জন্য নিয়মকানুন আরও কঠোর এবং আঁটোসাঁটো হল। আগের অধ্যায়ে আলোচিত ইউনিভার্সিটি অফ লন্ডন এবং রয়্যাল কলেজ অফ ফিজিশিয়ানস-এর প্রশ্নপত্রগুলো স্মরণ করে আমরা কলকাতা ইনিভার্সিটির নতুন নিয়মকানুনগুলোকে দেখি।
নিয়মাবলী
এমবি ডিগ্রির জন্য একজন ক্যান্ডিডেটকে First Examination in Arts পাস করতেই হবে, এবং পাসের পরে কোন স্বীকৃত মেডিক্যাল কলেজে ৫ বছর পড়াশুনো করা বাধ্যতামূলক। পরীক্ষা পাসের সার্টিফিকেট দাখিল করতে হবে।
(১) “Descriptive and Surgical Anatomy, Chemistry, Materia Medica, General Anatomy, Botany, Comparative Anantomy and Zoology, Surgery, Midwifery, Medical Jurisprudence and Diseases of the Eye”-এর লেকচার অ্যাটেন্ড করতে হবে।
(২) প্র্যাক্টিক্যাল ফার্মেসি অধ্যয়ন করতে হবে।
(৩) ৩টি winter terms-এ অন্ততপক্ষে ১২টি ডিসেকশন করতে হবে।
(৪) “সার্জিকাল রিজিওন” ডিসেক্ট করতে হবে, এবং ২টি winter terms-এ সার্জিকাল অপারেশন বাধ্যতামূলক।
(৫) ৬টি প্রসব করানো বাধ্যতামূলক।
(৬) স্বীকৃত হাসপাতালে ৩ মাস আউটডোর ডিসপেনসারিতে, ১৫ মাস সার্জিকাল প্র্যাক্টিসে, ১৫ মাস মেডিক্যাল প্র্যাক্টিসে এবং ৩ মাস চোখের বিভাগে প্রশিক্ষণ নিতে হবে।
(৭) তাকে দুটি মেডিক্যাল পরীক্ষায় পাস করতে হবে – প্রথমটি, তৃতীয় বর্ষের শেষে (ডেসক্রিপটিভ এবং সার্জিকাল অ্যানাটমি, কেমিস্ট্রি, বোটানি, মেটেরিয়া মেডিকা ও ফার্মেসি, এবং কম্প্যারেটিভ অ্যানাটমি ও ফিজিওলজির পরীক্ষা), এবং দ্বিতীয়টি, পঞ্চম বর্ষের শেষে (প্রিন্সিপাল অ্যান্ড প্র্যাকটিস অফ মেডিসিন, প্রিন্সিপাল অ্যান্ড প্র্যাকটিস অফ সার্জারি, অপথ্যালমিক মেডিসিন ও সার্জারি, মিডওয়াইফারি, মেডিক্যাল জুরিসপ্রুডেন্স ও টক্সিকোলজির পরীক্ষা)।
পরীক্ষা লিখিত, মৌখিক এবং প্রাক্টিক্যাল হবে। প্রথম পরীক্ষার জন্য পরীক্ষার ফি হিসেবে ১০ টাকা, এবং দ্বিতীয় পরীক্ষার জন্য পরীক্ষার ফি হিসেবে ২০ টাকা দিতে হবে। এখানে পাঠকদের স্মরণে আসবে লন্ডন ইউনিভার্সিটির নিয়ম ছিল পরীক্ষার ১৫ দিন আগে রেজিস্ট্রারের কাছে ৫ পাউন্ড ফি হিসেবে দিতে হত। (GRPI 1863-64, পৃঃ ২৫-২৬)
অনার্স পরীক্ষায় তারাই যোগ্য বলে বিবেচিত হত যারা এমবি পরীক্ষায় প্রথম বিভাগে পাস করেছে। এদের পরীক্ষা নেওয়া হত – সার্জারি, মেডিসিন, মিডওয়াইফারি, এবং মেডিক্যাল জুরিসপ্রুডেন্সে। লিখিত এবং প্র্যাক্টিক্যাল পরীক্ষা হত।
ডক্টর ইন মেডিসিন তথা এমডি পরীক্ষার জন্য একজন ছাত্রকে আর্টস এবং মেডিসিন দুটি বিষয়েই গ্র্যাজুয়েট হতে হত। এমবি পরীক্ষা পাস করার পরে হয় সে ৫ বছর “certified practice of the Medical profession” কিংবা “two years Hospital practice and two years private practice” অথবা “two years practice, either hospital or private, if the candidate be a graduate in Medicine with Honors” – এই শর্তগুলো পূরণ করতে হত।
তাকে পরীক্ষার ফি হিসেব ১০০ টাকা দিতে হত। যেসব বিষয়ে তাকে পরীক্ষায় পাস করতে হত সেগুলো হল – মেডিসিন, সার্জারি, মিডওয়াইফারি, এবং হাইজিন ও প্যাথলজি, (প্রাগুক্ত, পৃঃ ২৬-২৭)
আরেকটি বিষয়ও এসময় গুরুত্ব পেল। হাসপাতালে যে রোগীদের চিকিৎসা হচ্ছে তাদের nosological শ্রেণীবিভাগ।
(মেডিক্যাল কলেজের ইনডোর রোগীদের ক্ষেত্রে ১৮৬৬-৬৭ সালের হিসেব)
মেডিক্যাল কলেজের কৃতী গবেষকদের গবেষণাপত্র
১৮৬৩ সালের ২৭ মে সুর্য গুডিভ চক্রবর্তী একটি প্রবন্ধ লেখেন “Necessity of Forming A Medical Association in Bengal Medical Gaculty of Calcutta University”। (Chuckerbutty, Popular Lectures on Subjects of Indian Interest, 1870, পৃঃ ১২২-১৩৬) এ লেখায় তিনি প্রথম বাংলায় ব্রিটিশ মেডিক্যাল অ্যাসোসিয়েশনের বাংলা শাখা তৈরির প্রস্তাব দেন। এরপরেই ১৮৬৪ সালে ব্রিটিশ মেডিক্যাল অ্যাসোসিয়শের বেঙ্গল ব্র্যাঞ্চ খোলা হয়েছিল তাঁরই বিশেষ উদ্যোগে। তাঁর এই প্রবন্ধেই তিনি মেডিক্যাল কলেজ থেকে পাস করা ও প্রশিক্ষিত এবং অ-প্রশিক্ষিত (আয়ুর্বেদ, ইয়ুনানি, হেকিমি, জড়ি-বটির সাহায্যে যারা চিকিৎসা করেন) চিকিৎসার বিভাজন রেখার প্রসঙ্গকে জোর দিয়ে বলেন। এবং পাস করা, প্রশিক্ষিত ডাক্তারদের লাইসেন্স বা রেজিস্ট্রেশন বাধ্যতামূলক করার প্রস্তাব রাখেন। আজকের রেজিস্টার্ড মেডিক্যাল প্র্যাক্টিশনার্স-এর আদিরূপ ছিল এই উদ্যোগ।
এ লেখাতে তিনি বলেন যে কলকাতা বিশ্ববিদ্যালয়ের মেডিক্যাল ফ্যাকাল্টির বড় ত্রুটি হল ২টি ব্যতিক্রম বাদ দিয়ে “all its members are Europeans, with little knowledge of vernaculars and of the opinions, feelings, wishes, habits and customs of the natives. The result is that practically it represents European opinions and interests, and ignores national element.” (Popular Lectures on Subjects of Indian Interest, পৃঃ ১৩৫) এ কথাগুলোর প্রতিটি শব্দই গুরুত্বপূর্ণ। ইউরোপীয় শিক্ষা গ্রহণ করে তাকে “দেশীয়করণ” করার ইঙ্গিত রয়েছে চক্রবর্তীর বক্তব্যে।
বেঙ্গল ব্র্যাঞ্চের প্রথম মিটিংয়ে মহেন্দ্রলাল সরকার একটি প্রবন্ধ পাঠ করেন “A Case of Hepatic Abscess” শিরোনামে। প্রবন্ধটি পরে ব্রিটিশ মেডিক্যাল জার্নাল-এ (জুলাই ৯, ১৮৬৪, পৃঃ ৩৬-৩৭) প্রকাশিত হয়। তিনি বলেন – “আমি এই কেসটি সবার সামনে এনেছি সবার মতামতের জন্য – on the opening hepatic abscess externally.” (পৃঃ ৩৭) সেসময় পরস্পরের সাথে নতুন কেস নিয়ে আলোচনা এবং মত বিনিময়ের একটি প্রাণবন্ত ধারা ছিল, এমনটা অনুমান করা যায়।
এর বাস্তব প্রমাণ মেলে ইন্ডিয়ান মেডিক্যাল গেজেট-এ প্রকাশিত “Meetings of the Bengal Branch of the British Medical Association” রিপোর্টে। রিপোর্টটিতে বলা হয় – “Dr. Chuckerbutty brought forward a case of empyema of the right pleura, with abscesses in the liver and spleen … In connection with this case, Dr. Chuckerbutty made some remarks on the pathology of cholera”। এ ছাড়াও আরও কিছু কেস নিয়ে তিনি আলোচনা করেন। রিপোর্টে উল্লেখ করা হয় – ডঃ রবসন এবং গোপালচন্দ্র রায় আলোচনায় অংশ নিয়েছিলেন। এ ছাড়া লালমাধব মুখার্জি “described a case of tetanus following an injury to the calf of the leg received a month before. The case became steadily worse, until 150 large l’ound worms were passed from the bowels, when the symptoms began to abate.” (“Meetings of the Bengal Branch of the British Medical Association”, Indian Medical Gazette, আগস্ট ১, ১৮৬৭, পৃঃ ২০৬)
ব্রিটিশ মেডিক্যাল জার্নাল-এ (সেপ্টেম্বর ১০, ১৮৬৪, পৃঃ ২৯৯-৩০০) প্রকাশিত হল সূর্য গুডিভ চক্রবর্তীর পেপার “A Case of Amyloid Degeneration”। এ পেপারে তিনি পোস্ট-মর্টেম পরীক্ষার ফলাফল হিসেবে জানান যে Amyloid টিস্যু/কোষ পাওয়া গিয়েছে সেগুলোতে আয়োডিন যোগ করলে হলদে-বাদামি রঙ নিচ্ছে। আয়োডিন দেবার অব্যবহিত পরে সালফিউরিক অ্যাসিড দিলে সাময়িকভাবে বেগুনি কিংবা নীলচে রঙ নিচ্ছে। মেডিক্যাল কলেজের কেমিক্যাল ল্যাবরেটরিতে কানাইলাল দে “found objects which closely resembled the arrow-root starch-corpuscles”। (পৃঃ ৩০০) এ পেপারটি থেকে মনে হয় ভির্শোর আবিষ্কৃত cell pathology-র আধুনিক ধারণা চক্রবর্তী গ্রহণ করেছেন। ১৮৬৭ সালে তাঁর পেপার প্রকাশিত হল ইন্ডিয়ান মেডিক্যাল গেজেট-এ – “On the Pathology of Hepatic Abscess as a Result of Dysentery”। (Indian Medical Gazette, 1867 Sep 2; 2(9): 222–223) ব্রিটিশ মেডিক্যাল জার্নাল-এ ২ কিস্তিতে প্রকাশিত হয়েছিল তাঁর পেপার “The Present State of Medical Profession in India” (জুলাই ২৩, ১৮৬৪, পৃঃ ৮৬-৮৮, এবং জুলাই ৩০, ১৮৬৪, পৃঃ ১০৯-১১২)
এর আগে তাঁর পেপার “Iodide of Potassium in the treatment of Aneurism” (British Medical Journal (BMJ), 2, 81(1862), 61-64, BMJ, 2, 82 (1862), 85-86) প্রকাশিত হয়েছিল। Iodide of Potassium-এর সাধারণভাবে ব্যবহার ছিল মূলত যে সমস্ত অঙ্গের অভ্যন্তর ফাঁপা, যেমন scrotum বা arterial aneurysm কিংবা in cases of bronchocele or thyroid gland, সেগুলোকে সাইজে ছোট করার কাজে। চক্রবর্তী এর বাইরে ভিন্ন ক্ষেত্রেও Iodide of Potassium-এর ব্যবহার করেন।
১৮৬৮-৬৯ শিক্ষাবর্ষ থেকে ১৮৭২-৭৩ শিক্ষাবর্ষের আলোচনা
১৮৬৮-৬৯ শিক্ষাবর্ষের রিপোর্ট পেশ করেন কলেজের প্রিন্সিপাল Chevers। এ রিপোর্টে উল্লেখ করার মতো ঘটনা হল (যে গতানুগতিকতায় রিপোর্ট পেশ করা হয়ে থাকে তার বাইরে) – (১) গত সেশনে এমবি পরীক্ষায় উত্তীর্ণ ৪ জন পরীক্ষার্থীকে ইউনিভার্সিটির বার্ষিক কনভোকেশনে (ফেব্রুয়ারি মাসে) ডিগ্রি দেওয়া হয়েছে। এ ৪ জন ছাত্র হল – কালীপদ গুপ্ত, C. T. Peters, ফকিরচন্দ্র ঘোষ এবং নবকুমার বন্দ্যোপাধ্যায়। (GRPI 1868-69, Appendix A, পৃঃ ৪৫৩) এবং (২) Chevers হৃষ্টচিত্তে ঘোষণা করেন (এর আগে মেডিক্যাল কলেজে যে eleemosynary তথা দাতব্য/ভিক্ষার উপরে নির্ভরশীল শিক্ষাদানের প্রথা চালু ছিল তাকে অতিক্রম করে) – “year by year, the College continues progressively to emerge more and more from its original state of absolute dependence upon Government for pecuniary support.” (GRPI 1868-69, Appendix A, পৃঃ ৪৫৯)
১৮৬৯-৭০ শিক্ষাবর্ষের রিপোর্ট পেশ করেন যথারীতি কলেজের প্রিন্সিপ্যাল Chevers। রিপোর্টে বলা হয় যে ১৮৬৮ সালে নতুন নিয়ম করা হয়েছিল – বেঙ্গলি ক্লাসের ছাত্ররা বাধ্যতামূলকভাবে মেডিক্যাল কলেজে ভর্তি হবার আগে ২ বছর সিভিল ডিসপেনসারি বা রেজিমেন্টাল হাসপাতালে শিক্ষানবিশী করতে হবে। এর পরিণতিতে, ১৮৬৯-৭০ শিক্ষাবর্ষে বেঙ্গলি ক্লাসে ৩৮ জন কমে গেছে। (GRPI 1869-70, পৃঃ ২৮) কিন্তু এ শিক্ষাবর্ষেই বেঙ্গলি ক্লাসের জন্য কেমিস্ট্রি এবং মেডিক্যাল জুরিসপ্রুডেন্স শিক্ষার ব্যবস্থা করা হল। এর কারণ হল “practical knowledge of native doctors in the interior of districts in regard to the medico-legal questions that constantly arise in judicial investigation” গুরুত্বপূর্ণ ভূমিকা নেয়। (পৃঃ ২৮-২৯)
এমবি পরীক্ষায় উত্তীর্ণ ২ জন পরীক্ষার্থীকে ইউনিভার্সিটির বার্ষিক কনভোকেশনে (ফেব্রুয়ারি মাসে) ডিগ্রি দেওয়া হয়েছে। এরা দুজন হল – ঈশানচন্দ্র দে এবং পূর্ণচন্দ্র চক্রবর্তী। (GRPI 1869-70, Appendix A, পৃঃ ৩১৪) একটি নতুন “Student Apprentice Class” খোলা হল। যদিও এই ক্লাসটি “at present subject of correspondence between the Director of Public Instruction and the Government”-এর স্তরে রয়েছে। এবং ক্লাসটি এখনও যথেষ্ট সফল হয়নি। (প্রাগুক্ত, পৃঃ ৩১৫) হাসপাতালে চিকিৎসিত রোগীর সংখ্যা ৪২,৪৩২। (পৃঃ ৩২০)
১৮৭২-৭৩ শিক্ষাবর্ষে মেডিক্যাল কলেজ নিয়ে বেশি কথা খরচ করা হয়নি। বলা হয়েছে – “মেডিক্যাল কলেজে প্রবেশাধিকার এখন যেকোন ছাত্রের জন্য অবাধ, যদি সে ছাত্র ইউনিভার্সিটি এন্ট্রান্স এগজামিনেশন পাস করতে পারে। ৩০ মার্চ ১৮৭৩-এ কলেজের ছাত্রসংখ্যা ২৯৫ হন। ১৮৭২ সালে এ সংখ্যা ছিল ২৪৭।” এখানে সম্ভবত ইংরেজি ক্লাসের কথা বলা হয়েছে। এরপরে যে গুরুত্বপূর্ণ কথা বলা হয় তাহল – “The cost of this department was Rs. 1,23,030, of which Rs. 1,05,115 was defrayed by State grants and Rs. 17,914 from fee receipts.” বছরে প্রতিটি ছাত্রের জন্য গড়ে খরচ হয় ৩৮১ টাকা করে, এবং এটা ছাত্রসংখ্যার ওপরে নির্ভর করে। (GRPI 1872-73, পৃঃ ১৭) এই রিপোর্ট থেকে জানা যাচ্ছে, ১৮৭২ সালের মেডিক্যাল এগজামিনররা কলকাতা বিশ্ববিদ্যালয়ের সিন্ডিকেটের কাছে তাঁদের Resolution হিসেবে পাঠাচ্ছেন – “(1) That the First Examination in Arts should be substituted for the Entrance Examination as a qualification for admission to the First L.M.S Examination, (2) every candidate for the Second M.B Examination should (in addition to the present subjects) be examined in one of following subjects to be selected by himself: – Chemistry, Botany, Comparative Anatomy and Zoology, Physiology (including Comparative Anatomy)”। (প্রাগুক্ত, পৃঃ ১৭)
মেডিক্যাল কলেজের বেঙ্গলি এত বেশি ছাত্র তখন ভর্তি হচ্ছে যে সিদ্ধান্ত নেওয়া হয়েছিল “removing the Bengali classes from the Medical College and locating them at Sealdah … Dr. Woodford, the Professor of Medical Jurisprudence in the Medical College, who has been in charge of the Sealdah Hospital, is put at the head of the school now attached to it”। (প্রাগুক্ত, পৃঃ ১৮) ক্যাম্পবেল মেডিক্যাল কলেজের (বর্তমানে নীলরতন সরকার মেডিক্যাল কলেজ) ভিত্তিপ্রস্তর তৈরি হল।
নার্স তথা আধুনিক ধাই তৈরির উদ্যোগ
ইন্ডিয়ান মেডিক্যাল গেজেট-এ একটি প্রতিবেদনে বলা হয়েছিল – “Sub-Assistant Surgeons have, for some time past, been instructed in midwifery; and one of these, a proficient in the art, is now appointed at the Medical College, in Calcutta, to teach the Native Doctor class; so that there is a prospect of the blessings of good midwifery, as well as of good medicine and surgery, being, in course of time, conveyed to the masses. But this, in itself, will do nothing towards the safe delivery of poor Native women in their own homes in remote villages, miles and miles away from dispensaries and Sub-Assistant Surgeons and Native Doctors. Though, indeed, when Native Doctors generally are educated with a view to their establishing themselves in practice, as some of those of the Bengalee class in the Medical College have done, then this desirable result may come to pass.” (“Native Midwifery” Indian Medical Gazette, October 1, 1968, পৃঃ ২৩৯)
মোদ্দা কথা হল, মেডিক্যাল কলেজের ছাত্রদের ধাত্রীবিদ্যায় প্রশিক্ষণ দেবার কাজ বেশ অনেক বছর ধরেই চলছে। পরে বেঙ্গলি ক্লাসের নেটিভ ডাক্তারদেরও এ প্রশিক্ষণ দেওয়া হয়। কিন্তু এগুলো “will do nothing towards the safe delivery of poor Native women in their own homes in remote villages, miles and miles away from dispensaries and Sub-Assistant Surgeons and Native Doctors”। তাহলে উপায় কি? যদি যে ধাইয়েরা এতদিন প্রসব করিয়ে এসেছে তাদের ধাত্রীবিদ্যায় কিছুটা প্রশিক্ষিত করা যায় তাহলে অনেক কম খরচে বৈজ্ঞানিকভাবে প্রসব করানোর কাজটি করা সম্ভব। (দ্রষ্টব্য, West Bengal State Archives, General Department, Medical Branch, November 1871, Proceedings 38–43)
১৮৭০-এর ডিসেম্বরে “a candidate came forward for the training।“ (অম্বালিকা গুহ, Colonial Modernities: Midwifery in Bengal, c. 1860-1940, 2018, পৃঃ ৭২) পরবর্তীতে আরও অনেক মহিলা এগিয়ে আসে, এত সংখায় যা ধারণক্ষমতার চেয়ে বেশি। ইংরেজি এবং বাংলা সংবাদপত্রে খবরটি বিজ্ঞাপিত হয় “with the help of Brahmo leaders like Keshab Chandra Sen.” (প্রাগুক্ত, পৃঃ ৭২)
৭ জুন, ১৮৬৭ সালে স্বয়ং ফ্লোরেন্স নাইটিংগেল লেখেন – “in the Medical College Hospital at Calcutta, where it was founded, the Eurasian women who before would not lay their hands to anything, when they saw the Englishwomen doing it, began to do it too. And the Eurasian matron and Eurasian nurses make a very tidy staff now at Calcutta Medical College Hospital.” (Florence Nightingale on health in India, ed. Gerard Vallee and Lynn McDonald, 2006, পৃঃ ৯৫৬) সহজ কথা হল, হয় নতুন মহিলাদের নার্স হিসেবে প্রশিক্ষণ দেওয়া হোক কিংবা শহুরে না গ্রামীণ ধাইদের প্রশিক্ষিত করা হোক। অর্থাৎ ফ্লোরেন্স নাইটিংগেলের মতো ব্যক্তিত্বের তরফেও মেডিক্যাল কলেজে নার্সিং ট্রেনিং চালু করার একটি পরোক্ষ চাপ ছিল।
এরকম এক পরিপ্রেক্ষিতে ১৮৭০ সালে সরকারের তরফে সিদ্ধান্ত নেওয়া হয় যে ভারতীয় মহিলাদের নার্স হিসেবে প্রশিক্ষিত করার জন্য মেডিক্যাল কলেজে ক্লাস নেওয়া হবে। ১৮৭১ সালে ১০ জন ট্রেনিং-এর জন্য যোগদান করে। পরীক্ষায় ৪ জন পাস করে, একজন প্রশংসনীয় কাজ করে। (Centenary, পৃঃ ৪৬) মেডিক্যাল কলেজের আরেকটি নতুন শাখা প্রসারিত হল।








মেডিকাল কলেজের মতন গুরুত্বপূর্ণ প্রতিষ্ঠানের ইতিহাসের এরকম তথ্যসমৃদ্ধ এবং চিন্তার খোরাক জোগান প্রবন্ধের জন্য লেখক ডঃ ভট্টাচার্য্যকে ধন্যবাদ।
Dear Jayanta — I am late by a day to scan your latest on — continuing serial on “History of CMCH”– in the pages of Doctors Dialog. The natural empathy and whole hearted loving involvement of the early English teachers — be it Medicine or any other field of the then happening days of Western Education — is legendary. All and Everything was BAD involving westerners is slogan of DESHBHAKTS — for a purpose , well known to any ” thinking / Introspecting mind. In old CMCH – Vellore — I had been fortunate to get that type of –dealings and shored up feelings — from western missionaries. Interestingly — one of my direct mentor– Prof. Arnold Fitzgerald Desmond (a blue eyed Irishman) — was born in Eden Hospital,Calcutta and trained in Madras Stanley Medical College — speaking fluent Bengali — having been a son of Missionary stationed in Gosaba (Sunderban) during Hamilton days. Your description of the manner and character of those early dedicated teachers — both native and european — would sound as an ” Anathema — in Ayushman days”. Best Wishes — Good Goings– n.da
অত্যন্ত গুরুত্বপূর্ণ একটি লেখা। দারুণ।
এই অনবদ্য লেখনী গুলি না পড়লে মেডিক্যাল কলেজের ইতিহাস কোনোদিন জানা হতো না, অসংখ্য ধন্যবাদ
চিকিৎসাবিজ্ঞান শেখা আগেই শুরু হয়েছে। এবার শিক্ষণ ব্যবস্থার সুপরিকল্পিত নিয়মাবলী ও ব্যবহারের চিন্তা শুরু হল।
সৈনিক স্বার্থ দেখতে চাওয়াটা অবশ্যই সাম্রাজ্যবাদী প্রয়োজনে শুরু হয়েছিল, কিন্তু এ দেশে চিকিৎসাব্যবস্থার অগ্রগতি এর জন্যই সম্ভব হয়েছিল। অসুস্থ সৈনিকদের বিষয়ে যে দুটি সারণী পেশ করা হয়েছে তা থেকে এটা স্পষ্ট যে ব্রিটিশ সৈনিকদের লাগামহীন জীবনে কোন বিধিনিষেধ ছিল না।
সৈনিকদের রোগ না হতে দেওয়ার স্বার্থে যে স্যানিটেশনের ওপর জোর দেওয়ার প্রয়োজন এটাও উপলব্ধি করা শুরু হল।
নার্স বা ধাত্রীদের প্রয়োজনীয়তা বুঝে তাদের জন্যও শিক্ষাক্রম শুরু করাও একটি ঐতিহাসিক পদক্ষেপ।
কলকাতা মেডিকাল কলেজ অবশ্যই ভারতে আধুনিক চিকিৎসাবিজ্ঞানের শুরু এবং অগ্রগতির আদি পীঠস্থান।
চমৎকার লেখা। নমস্কার ও অভিনন্দন ডঃ জয়ন্ত ভট্টাচার্যকে। আপনার লেখাগুলো পড়ে সমৃদ্ধ হচ্ছি।