This pandemic has overwhelmed both public and private healthcare system as it struggles to find the correct balance between covid and non covid patients within the existing shortage of both hospital beds and doctors. But such generalization involving ‘quantity’ tends to overlook the relative lack of access to ‘quality’ healthcare in majority private and public health set-up due to scarcity of trained human resources and optimum infrastructure. This is the natural outcome of State modus operandi of promoting dual mix of public – private healthcare since 1990s, based on an economic understanding that ‘quality’ healthcare is a non-essential luxury commodity (like cosmetics, cars, jewellery, etc.) and extent of accessibility should be determined by the ability to afford at market prices in a private setting. That means the public and small private healthcare sector catering the majority poor does not have the required infrastructure and human resources to deliver ‘quality’ optimal service. That leaves behind the big private health sector (i.e. corporate sector or big nursing homes) which is supposed to provide ‘quality’ treatment to the people who can afford.
Current corona pandemic and nation-wide rationing of such ‘quality’ private healthcare facilities for ‘select few’ has exposed this State bankruptcy once and for all. But the State still remains in denial of the very basic nature of the problem arising out of such commodification of healthcare for profit that has left the ‘majority poor’, both covid and non covid patients at the mercy of already strained sub-optimal ‘quality’ small private and public health-care facilities, while tactfully diverting the blame on Muslims and China.
THE MODUS OPERANDI
- Diversion of State resources from public to private sector so as to create conditions to curtail both ‘quantity’ of beds and doctors along with ‘quality’ of treatment in State-run hospitals and health care centres.
The State in its commitment to bridge the gap of both required ‘hospital beds’ and ‘doctors’, started to shift the major onus on to the private sector. This started with private practice restrictions during the 1990s to push the best doctors (and many of them fantastic teachers) out of government teaching hospitals. The diversion created a separate elite ‘pool of doctors’ that helped the private sector expand at the expense of public sector. The State in fact wanted to restrict their role of providing treatment to just the poor who cannot afford private sector. The success of such modus-operandi required State apathy towards public health care system in terms of both ‘quantity’ and ‘quality’ of healthcare delivery. This remains the main driving force which helped the private health sector flourish over the last three decades as the Indian State gambled away the fate of our entire healthcare delivery system to the private players which now caters to 60% of all IPD patients and 80% of all OPD patients.The health budgetary allocations in fact, continue to stagnate at around 1% since 1990s. The State sponsored insurance schemes like Ayushman Bharat (Central government) and Sasthya Sathi (State government), etc. which covers inpatient tertiary care expenses in private sector for people living below poverty line have further diverted such precious State funds into the hands of insurance companies and private health sector since 2008.
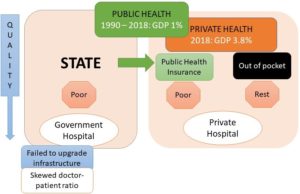 Figure 1: Diversion of State resources from public to private sector
Figure 1: Diversion of State resources from public to private sector
The MOHFW 2018 data validates such diversion of State resources as there is still just one government hospital bed per 1,844 population and one state-run hospital for every 55,591 population. KPMG, 2016 report states that 37% of rural India don’t have access to IPD facilities within 5 km distance and 68% don’t have access to OPD facilities. But such generalization involving ‘quantity’ tends to overlook the relative lack of access to ‘quality’ healthcare in existing State-run hospitals. The 3-tier primary healthcare services consisting of sub-centres (SCs), primary health centres (PHCs), community health centres (CHCs) are the worst affected. MOHFW 2018 data revealed that out of such 156,231 SCs, 78,569 were without male health workers, 6,371 without auxiliary nurse midwives and 4,263 without either. PHCs are the source of first contact with doctors, and suffer from shortage of 3,027 doctors to achieve a minimum 40% patients per day out patient care as per Indian Public Health Standards (IPHS). 1,974 PHCs are in fact without doctors, leaving behind 12% of all patients without access to primary health care each day. Overall, only 11% SCs, 13% PHC and 16% CHCs in rural India meet IPHS standards. That means the secondary (district hospitals, and block community health centres) and the tertiary care centres (medical colleges and super-speciality hospitals) are over-burdened due to unnecessary referral of patients, which in turn follows a similar pattern of scarcity and sub-optimal treatment.
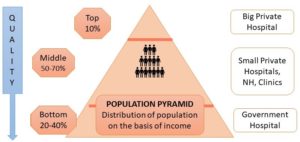
Figure 2: Population pyramid (based on distribution of income) suggests that 60-80% of population is dependent on private health sector and quality of treatment decreases in accordance to affordability
(to be continued)